Stereotyping and stigmatising disability: A content analysis of Canadian print news media about fetal alcohol spectrum disorder
John Aspler, Neuroethics Research Unit, Institut de recherches cliniques de Montréal
john [dot] aspler [at] ircm.qc.ca
Natalie Zizzo, Biomedical Ethics Unit, Experimental Medicine, McGill University
Nina Di Pietro, Faculty of Humanities and Social Sciences, Department of Psychology, Douglas College
Eric Racine, Department of Medicine and Department of Social and Preventive Medicine, Université de Montréal and Department of Neurology and Neurosurgery, Experimental Medicine, McGill University
Abstract: People with fetal alcohol spectrum disorder (FASD), a complex and controversial neurodevelopmental disability caused by alcohol exposure in the womb, report experiences of stigma in different parts of their lives. The media, sometimes central to how a public understands and constructs marginalized identities, have a notable history of poorly representing people with disabilities like FASD (including in Canada), which could increase their stigmatisation. Additionally, given its cause, women who drink while pregnant can also face stigmatisation – with some public discourses evoking narratives that promote blame and shame. To gain insight into the kinds of information presented to Canadians about FASD, alcohol, and pregnancy, we conducted a media content analysis of 286 articles retrieved from ten of the top Canadian newspapers (2002-2015). In this article, we report key themes we identified, most common being ‘crime associated with FASD’. We explore connections between this coverage, common disability stereotypes (i.e., criminal behaviour and ‘the villain’), FASD stigma, and expectations of motherhood.
Keywords
- stigma
- stereotypes
- disability
- fetal alcohol spectrum disorder
- FASD
- alcohol and pregnancy
- media content analysis
- motherhood
Stereotyping and stigmatising disability: A content analysis of Canadian print news media about fetal alcohol spectrum disorder
John Aspler, Neuroethics Research Unit, Institut de recherches cliniques de Montréal
john [dot] aspler [at] ircm.qc.ca
Natalie Zizzo, Biomedical Ethics Unit, Experimental Medicine, McGill University
Nina Di Pietro, Faculty of Humanities and Social Sciences, Department of Psychology, Douglas College
Eric Racine, Department of Medicine and Department of Social and Preventive Medicine, Université de Montréal and Department of Neurology and Neurosurgery, Experimental Medicine, McGill University
Introduction
Stigmatisation, a process of negative stereotyping that can cause discrimination, remains a tremendous social challenge and a barrier to the wellbeing of marginalized populations. Link and Phelan (2001) describe stigmatisation as a process involving the “co-occurrence” of several key components: group differences deemed salient by a given society become fodder for stereotyping, othering, and discrimination in a context where various forms of power align against a particular group. Public attitudes toward – and narratives about – a group can impact how societies understand, perceive, and support them. In this paper, we focus on how common media stereotypes could contribute to the stigmatisation of two such groups: 1) people with a neurodevelopmental disability called fetal alcohol spectrum disorder (FASD); and 2) women who drink while pregnant. We analyzed Canadian print news media about FASD and drinking during pregnancy to better understand the information readily accessible to many Canadians.
What does a diagnosis of FASD entail, medically and socially?
FASD, a complex and controversial diagnosis, results from fetal exposure to alcohol in utero (Cook et al. 2016; Chudley et al. 2005). When the diagnosis first emerged, it was initially attributed to children of “chronic alcoholic women” (Jones et al. 1973); however, the diagnosis soon expanded to encompass a wider spectrum of potentially affected individuals (Armstrong 1998; Koren et al. 2003). FASD presents heterogeneously; it can present with or without facial features, and may affect executive function, behaviour, and cognition, among other “brain domains” (e.g., motor function, language) (Cook et al. 2016; Chudley et al. 2005). These differences are sometimes referred to as “primary disabilities” in the medical literature (Koren et al. 2003), meaning “those that reflect the [central nervous system] dysfunctions inherent to the… diagnosis” (Streissguth et al. 1996). Recent Canadian diagnostic guidelines categorize FASD as: 1) FASD with sentinel facial features; 2) FASD without sentinel facial features; and 3) an at-risk category that does not yet indicate diagnosis (Cook et al. 2016). To be diagnosed, an individual must present with deficits in three of ten key “brain domains” and should typically have confirmed prenatal alcohol exposure. Ultimately, FASD is a difficult-to-assess diagnosis that requires diagnostic evaluation by a large multidisciplinary team – including physicians, speech language pathologists, social workers, and others.
The “primary disabilities” of FASD can be distinguished from more complex “secondary disabilities”[1], which include social sequelae and issues like homelessness, criminal behaviour, and substance abuse (Streissguth et al. 1996). While primary disabilities have been described as arising directly from neurological damage caused by alcohol, secondary disabilities relate to how people with FASD integrate into society as they age because of their primary disabilities[2].
Importantly, people with FASD have reported facing problems such as social exclusion, poor support systems, and employment discrimination (Salmon and Buetow 2012; Stade et al. 2011), which constitute potential consequences of the stigmatisation process described by Link and Phelan (2001). Additionally, women who consume alcohol during pregnancy can face stigmatisation given the connection between alcohol and an FASD diagnosis (Eggertson 2013; Salmon 2008; Abadir and Ickowicz 2016). For example, public discourse and health messages that emphasize blame, shame, and a mother’s individual responsibility can feed into stereotyped portrayals of women who drink while pregnant as unfit, irresponsible, and even criminally negligent or evil mothers (Connolly-Ahern and Broadway 2008; Lowe, Lee, and Yardley 2010).
This study builds on previous media studies about FASD, alcohol, and pregnancy conducted in the UK (Lowe, Lee, and Yardley 2010), the US (Connolly-Ahern and Broadway 2008; Golden 2000), and Australia (Eguiagaray, Scholz, and Giorgi 2016; McCallum and Holland 2017). Each of these studies reported tensions around the construction of different and sometimes conflicting FASD stakeholder identities (e.g., people with FASD as victims of bad blameworthy birth mothers). Half of the studies had an explicit focus on alcohol and pregnancy over FASD itself. In principle, the Canadian context ought to bear similarities with the contexts previously studied given their related histories. For example, Australia and Canada have similar relationships to colonization and their treatment of Indigenous peoples, and one Australian study reported on Indigenous peoples in FASD coverage (Holland, McCallum, and Blood 2015). However, Canadian coverage merits its own investigation, given its potential impact on the construction and portrayal of FASD, and its interface with Canadian public health.
Disability stereotypes and stigmatisation in the media
The mass media, whether in the form of news, advertising, or entertainment, have a long history of poorly representing people with disabilities ( Barnes 1992; Day 2000; Devotta, Wilton, and Yiannakoulias 2013). Scholars have pointed to stereotyped portrayals of disability as potential sources of negative public attitudes, prejudice, and discrimination (Barnes 1992; Day 2000). In both fiction and news stories, people with disabilities can serve as one-dimensional narrative devices or objects used to evoke strong emotional responses in able-bodied audiences, rather than as complex and fully fleshed out individuals with their own experiences.
People with disabilities are often framed as victims or objects of pity (e.g., Tiny Tim in Charles Dickens’ A Christmas Carol: a sick child with a crutch), as burdens (e.g., Rain Man: an autistic man whose brother initially sees him as a burden), as super-heroic (e.g., Daredevil: a blind superhero with heightened senses), or as villainous (e.g., Richard the III in Shakespeare’s eponymous play has a curved spine, Joker in Batman: mentally ill and often confined to an asylum). These ideas do not just exist in fiction; many of these same stereotypes have been identified in Canadian newspapers (Haller et al. 2012), among other news media ( Barnes 1992). Given the heterogeneity of disabilities, these stereotypes “paint a rather distorted picture that is at odds with the way disabled people see themselves” (Day 2000). Ultimately, these stereotypes provoke concerns about cultural representations of individuals with disabilities and the impact of these stereotypes in generating and perpetuating a process of stigmatisation.
Like any complex or poorly understood disability, the FASD diagnosis itself could be a catalyst for stigmatisation; the group difference deemed salient is a set of symptoms attached to a diagnostic label, to which stereotypes could additionally be attached. However, unlike most other diagnoses, the impact of the FASD label spreads beyond the individual themselves, since a diagnosis of FASD may also tell us something about a biological mother’s behaviour.
Motherhood stereotypes and expectations in the context of alcohol consumption
Women regularly experience double standards, stereotypes, and gendered expectations about what it means to be a good person, woman, or mother (Armstrong 2003). For example, Ganong and Coleman (1995) describe the “American myth of motherhood”, which suggests that mothers are either “all good” (i.e., “perfectly loving, kind, patient, and giving”) or “all bad” (i.e., “rejecting, cold, and controlling”). They argue that this myth holds mothers responsible for their children’s wellbeing, while the role played by fathers is largely ignored. Essentially, in focusing on the behaviour of individual mothers, societies might then ignore social structures and social pressures that also contribute to these behaviours. Women who consume alcohol while pregnant could represent a strong case of the perceived “all bad” mother.
Exploring the history of Western attitudes toward women who consume alcohol, Carter (1997) explains that, in the United States in the late 1800s, women “who drank publicly or became drunk were considered sexually indiscreet and irresponsible mothers” [emphasis ours]. Even in the 1990s, women were still reduced to roles related to their sexual availability, or else their ability to reproduce and care for children (Carter 1997). Indeed, Armstrong (1998), in an article exploring the origin of the FASD diagnosis, points to major social changes during the 1960s-70s that generated “social distress about women’s propensity to act in ways that were independent of and perhaps in opposition to the maternal role as socially constructed”. She quotes Daniels (1993), who argues that “some women were not just [viewed as] bad mothers, but as ‘anti-mothers’ who violated their most fundamental natural instincts and who threatened to destroy the institutions of motherhood altogether”. Such historical context and shifting social roles (at least in the United States) reflected a growing “moral panic” surrounding alcohol use and pregnancy, which likely had an effect on North American reactions to the creation of the diagnosis of FASD (Armstrong and Abel 2000).
At the most basic level, stereotypes attached to the labels of ‘good’ or ‘bad’ mother could have a significant impact on public attitudes toward pregnant women. Some recent evidence even suggests that birth mothers of children with FASD are perceived as more blameworthy than other ‘bad’ women (e.g., incarcerated women) (Corrigan et al. 2017)[3]. In the end, the complex relationship between attitudes toward women, mothers, and children with disabilities leads to many possible sources of stigmatization in FASD (Bell et al. 2015).
In this paper, we explore Canadian print news media coverage of FASD. We focus on the portrayal of two key stakeholder groups: 1) people with FASD; and 2) women who drink while pregnant, with the aim of deconstructing stereotypes. We find that both individuals with FASD and mothers giving birth to children with FASD have been, at times, stigmatized as bad or as villains – consistent with previous literature (Connolly-Ahern and Broadway 2008; Dej 2011). However, Canadian print news media also contained some notable pushback against these stereotypes. We critically reflect on the connections between this coverage and problematic ways of constructing and portraying the identities of both people with disabilities and mothers.
Methods
In this study, we employed media content analysis (Macnamara 2005), similar to several previous studies conducted at our research unit (e.g., (Racine, Bar-Ilan, and Illes 2006)).
Sample
Using the Factiva news database, we searched for English and French print news articles published in Canada between January 1st 2002 and October 31st 2015, capturing media coverage from roughly the past fifteen years. We searched for the following keywords in headlines and lead paragraphs: “("fetal alcohol spectrum disorder" OR "FASD" OR "fetal alcohol syndrome" OR ("alcohol" AND "pregnancy") OR "ensemble des troubles causés par l’alcoolisation foetale" OR "ETCAF" OR "syndrome d’alcoolisation foetale" OR (“grossesse” AND “alcool”))”.
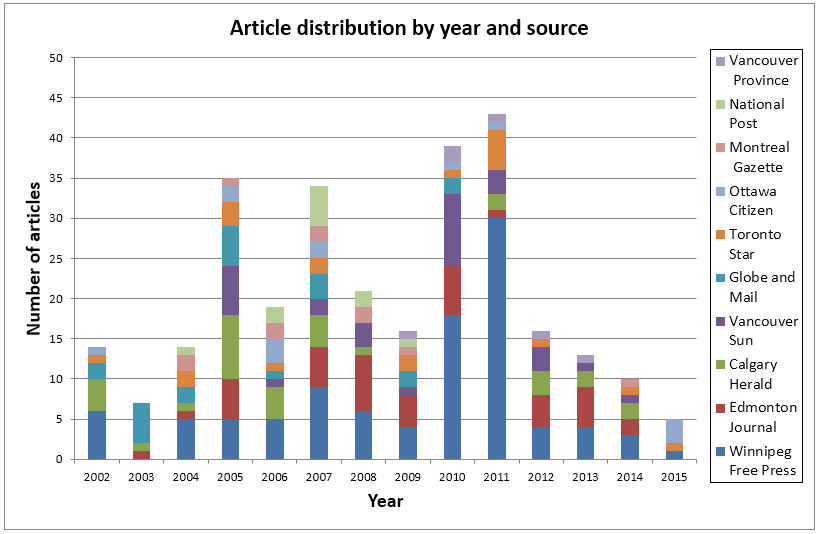
We restricted our search to ten of the most-distributed Canadian print news sources (Newspapers Canada 2009), all of which are available electronically: The Toronto Star (20), The Globe and Mail (22), The Montreal Gazette (11), The Vancouver Sun (30), The Vancouver Province (6), The National Post (11), The Winnipeg Free Press (100), The Calgary Herald (32), The Ottawa Citizen (13), and The Edmonton Journal (41)[4]. We excluded Le Journal de Montréal, La Presse, Le Journal de Québec, and The Toronto Sun because Factiva only began archiving these sources in 2011. See Figure 1 for more information about the distribution of the sample by year and by source.
Of the original 398 articles, we retained 286 after excluding: 1) articles we deemed to be irrelevant; 2) duplicates from the same source; and 3) short news briefs, which included synopses of several articles at once (not all FASD-related), summaries of articles already in the sample, and articles with too little content. Thirty-eight of the 286 retained articles were duplicates from different sources, which we included in our analysis to capture far-reaching messages.
Coding process
The initial coding guide was inductively developed by three coders using 25 randomly-selected articles from 2002-2011. We used NVivo (QSR International, Version 9.2.81.0) for coding and data analysis. Coder 1 then applied this guide to the remainder of the overall sample using a rich coding strategy (i.e., overlapping, non-mutually-exclusive codes). Coder 2 then conducted blind coding on another random sample of 25 articles to assess inter-coder reliability. Reliability was calculated in percent agreement for all main codes and sub-codes. Six codes and five sub-codes had percent agreement below 0.75 and were eliminated from the data. For quantitative analyses, we used individual articles as the sampling unit. After updating the sample to include articles published between 2012-2015, a fourth coder undertook a more detailed qualitative unpacking of the data, which led to further refinement of the coding guide. We then had a fifth coder conduct another round of blind coding on another random sample of 25 articles, to assess inter-coder reliability of the reorganized codes and sub-codes.
Coding Guide
We coded 286 articles for coverage of three broad categories: 1) scientific content; 2) clinical content; and 3) social content. This article reports on the eight codes (and eleven sub-codes) in the social content category (See Table 1). The scientific and clinical content will be reported elsewhere (Aspler et al. Under Review). Social content reflects discussions about the lives and needs of people with FASD and women who drink while pregnant. As the broadest category, categories included issues like crime, stigma and labelling, funding, and more.
Results
We identified eight major themes, or codes, (See Table 1) broken down across eleven sub-codes, with the most frequent being crime associated with FASD (37%, n=106). Table 1 describes the coding structure in detail and explains the scope of each code and sub-code with examples. In the text that follows, we provide a detailed overview of some of the richer and more complex themes. Illustrative examples are used to exemplify important qualitative aspects of the content, with key quotes provided in-text.
Table 1 – Results: Coding Structure, Percentage of Sample, and Illustrative Examples
| Code | Sub-code | Scope | % of sample # of articles | Examples |
| Crime associated with FASD | Article reports on crime associated with FASD | 37%, n=106 | ||
| Perpetrator of crime | Article reports on people with FASD as perpetrators of crimes; not always specific cases | 29%, n=83 | “A 14-year-old resident of a facility for youngsters diagnosed with FAS has been charged with first-degree murder in the case” (Calgary Herald 2002). | |
| Victim of crime | Article reports on people with FASD as victims of crime; not always specific cases | 8%, n=23 | “Two teenage boys suffering from [FASD] had been confined to makeshift cages fashioned from cribs and were beaten regularly...” (Toronto Star 2004). | |
| More support needed for FASD stakeholders | Article reports on the need for any kind of increased FASD support. Includes requests for specific programs and services, as well as broad calls for general support and funding. | 29%, n=82 | “Doctors dealing with the disorder say there is a dire need for more diagnostic services” (Toronto Star 2009). | |
| Awareness of FASD | Article reports on efforts to raise awareness about FASD and the impact of drinking while pregnant, and the need for greater awareness. Includes reports about current public awareness. | 28%, n=81 | “People from Norway House Cree Nation will walk and run to Winnipeg... to draw attention to FASD” (Winnipeg Free Press 2010). | |
| Family composition of people with FASD | Article reports on the family makeup of individuals with FASD. | 27%, n=73 | ||
| Adoptive families | Article reports on people with FASD who have been or might be adopted. Includes stories about children diagnosed and sometimes given up or placed in care long after adoption. Also includes calls for more support for adoptive parents. | 13%, n=38 | “The Jaffrays adopted [their children] when both were newborns with little inkling that they might suffer from FAS” (Toronto Star 2002). | |
| Foster Families | Article reports on children with FASD who live in or who may end up in the foster care system. Also includes concerns about foster families rejecting children with FASD, and how likely they are to remain in foster care compared to other populations. | 5%, n=15 | “He was diagnosed with fetal alcohol syndrome when he was two. In the past 15 year he’s lived in seven different foster and group homes” (Winnipeg Free Press 2006). | |
| Parents who have FASD | Article reports on people with FASD who have or who could have children; not always in reference to specific individuals. | 3%, n=10 | “Most will say it’s a cycle, and that a woman with many fetal alcohol-affected kids was born to a woman who drank while pregnant, too” (Winnipeg Free Press). | |
| Funding for FASD | Article reports funding for research, prevention, diagnosis, treatment, or other services. Includes calls for increased or better-directed funding, and complaints about current funding issues. Note that most referred to government funding in the western Canadian provinces of Manitoba, Vancouver, and Alberta. | 25%, n=72 | “Alberta’s decision to create a more co-ordinated system for dealing with FASD, and to hike spending to $10 million a year -- a $4-million increase -- is significant…” (Calgary Herald 2007). | |
| FASD and Indigenous populations in Canada | Article reports on Indigenous peoples and communities in Canada in the FASD context | 22%, n=62 | “About 48 per cent of aboriginal people strongly support a school screening program. That could be because FASD is widely seen as an aboriginal issue, even though it affects all groups” (Winnipeg Free Press 2011). | |
| Secondary disabilities associated with FASD | Article reports on secondary disabilities associated with FASD, sometimes explicitly using the term. | 21%, n=60 | “… people with FAS face daunting odds of dropping out of school, getting fired from jobs, becoming teenage parents, dabbling in drugs, tangling with the police and drifting in and out of homelessness” (Globe and Mail 2003). | |
| Substance abuse | Article reports on substance abuse or potential substance abuse by people with FASD | 7%, n=20 | ||
| Employment | Article reports unemployment or issues keeping a job for people with FASD | 5%, n=14 | ||
| Housing | Article reports homelessness or issues with independent living for people with FASD | 4%, n=11 | ||
| Inappropriate sexual behaviour | Article reports inappropriate sexual behaviour as a secondary disability of FASD. Excludes specific criminal cases featuring either a perpetrator or victim with FASD | 1%, n=4 | ||
| Impact of the social world on FASD | Article explores certain social factors that could impact or that could be impacted by FASD | 21%, n=59 | ||
| Stigma and Labelling | Article reports on the impact or the sources of stigma and labels associated with FASD on both people with FASD and women who drink while pregnant. | 12%, n=35 | “They almost never show clear signs of the facial dysmorphia that comes with FAS and spend their lives stigmatized for their unrecognized permanent brain damage” (Toronto Star 2005). | |
| Socioeconomic status | Article reports on socioeconomic status in the context of FASD | 9%, n=26 | “Its victims are often the children of poor mothers who suffer substance abuse and addiction” (Globe and Mail 2007). |
Crime associated with FASD
Perpetrator of crime – Criminal justice and culpability
Many articles coded here included explicit examples of crimes committed or allegedly committed by people with or suspected of having FASD (e.g., theft, arson, murder). Here, the media broadly framed people with FASD as either more likely to commit crimes than the average person or as comprising a disproportionate fraction of the Canadian inmate population. A few articles also discussed how the criminal justice system sometimes fails or does not appropriately accommodate people with FASD, as suggested in a 2012 article from the Edmonton Post: “‘…treatment availabilities while one is incarcerated, especially if overcrowding is an issue… are very, very minimal. The jails then become a bit of a dumping ground for problems in society that we haven’t been able to appropriately deal with’”.
Many articles also raised questions about the ways certain deficits associated with FASD could impact an individual’s moral or criminal culpability. For example, some suggested that these alleged perpetrators lacked insight into the consequences of their actions, as in a Winnipeg Free Press article from 2010: “…an older FASD teenager who appears normal often considers consequence -- while joining a gang or stealing a car -- in much the same way as a four-year-old”. In the case of minor offences, a lack of insight into consequences could reportedly lead to further trouble for these individuals (e.g., “…[people with FASD are susceptible to] charges, such as failure to appear, breach of probation or failure to comply with bail conditions… because of their struggles to stay organized and understand consequences” (Edmonton Journal 2013)). Some articles also suggested that consequence-based punishment like incarceration may not be effective for people with FASD if they have a deficit in understanding consequences.
In contrast, other articles focused an inability to assess the rightness or wrongness of their actions, as in this 2006 Winnipeg Free Press article: “and justice officials are trying to find a way to punish youths who often have no concept of right and wrong”. A final small set of articles suggested that, regardless of the ability to evaluate the morality of consequences or actions, the issue has to do with impulse control and intention: “‘He knows it’s wrong, but he doesn’t have the ability to self-regulate’” (Winnipeg Free Press 2011) or “‘He knew that it was wrong… but I hesitate to say that he knew that he wanted her dead’” (The Globe and Mail 2005).
Finally, these discussions about culpability explored the importance of considering a diagnosis of FASD as a mitigating factor during sentencing. Notably, some of these articles included perspectives that acknowledged potential deficits in understanding, but still privileged public safety over the needs of the accused (e.g., “What does society do with an habitual arsonist or a chronic car thief except jail them?” (Winnipeg Free Press 2010)).
Victim of crime
Most of these articles focused on stories of people with FASD as victims of crimes (e.g., of murder, of abuse), mostly about men or boys, although the few examples of female victims were typically about sexual assault or exploitation. A few articles discussed broader concerns about victimization, such as increased likelihood of people with FASD being victims of crime (e.g., “A famous research study on kids with FASD in the U.S. Pacific Northwest found 72 per cent of FASD kids studied had been victims of abuse” (Winnipeg Free Press 2011)), or problems faced in the criminal justice system, as in this Winnipeg Free Press article: “The prosecutor was warned the child [with FASD] would make a horrible witness [testifying against his father in a sexual abuse case] and couldn’t understand abstract questions… It resulted in the judge accusing the boy of lying and the father being released” (2011).
Family composition of people with FASD
Parent with FASD – Fathers and mothers with FASD portrayed differently
Some articles in our sample focused on the whole lifecycle, including what happened when individuals with FASD had children of their own. Many articles discussed how these children were cared for by other family members (e.g., grandparents) or were placed in foster or adoptive care. These stories typically discussed mothers with FASD, but a few focused on fathers with FASD. The articles about mothers included a mix of A) successful parenting stories: “[She] has a loving husband, three beautiful children and… a fetal alcohol spectrum disorder that affects her memory and her brain’s ability to get organized…” (Winnipeg Free Press 2011); and B) less successful stories, as in this 2012 Edmonton Journal article: “‘[She] is a very nice girl and is funny and can be very sweet at times’… But she is not fit to raise a child. The government agreed and the baby is in foster care”. All of the articles about fathers were framed positively and focused on overcoming hardship to live stable lives: “For more than a decade, [he] has been accompanied 12 hours a day, seven days a week, by a support worker from the Mennonite Central Committee. He now takes his girlfriend and 10-month-old daughter to work with him to keep him motivated” (Winnipeg Free Press 2006).
FASD and Indigenous populations in Canada
Many articles discussed concerns about increased prevalence of FASD in Indigenous populations compared to the general population in Canada. Several of those articles qualified that FASD has sometimes been incorrectly labeled an Indigenous-specific problem, since it can affect anyone. Several also discussed Indigenous people with FASD in the context of crime. Several more explored Indigenous awareness about FASD (e.g., “Aboriginals and adult women under 35 were the most likely to know the only cause of FASD is maternal drinking…” (Winnipeg Free Press 2011)), or Indigenous knowledge being used to prevent FASD (e.g., “…Mrs. Whiskeyjack has been trying to revive the ancient mentoring role of aboriginal seniors… And her attempts to help curb the reserve’s epidemic of fetal-alcohol syndrome seem to be working” (Vancouver Sun 2010)). Results about FASD-related discourse and Indigenous peoples in Canada are reported in a separate paper (Aspler et al. Under Review). Race and ethnicity were not typically discussed outside of Indigenous contexts in this sample.
Impact of the social world on FASD
Stigma and Labelling
Some articles outlined concerns about the impact of stigma on women who drink while pregnant, as in the case of this 2002 article from the Winnipeg Free Press: “Punishing these women is not helpful, it further stigmatizes and shames them, which keeps them from reaching out for support”. A few articles highlighted the positive impact the diagnostic label can have: “‘To a certain extent, it was a relief, because now I knew what the problem was’” (The Globe and Mail 2003), while others focused on the negative: “When he was younger, the Jaffrays were reluctant to push doctors to pin an FAS diagnosis on him, worried it would act as a self-fulfilling prophecy for a lifetime on the margins of society” (Toronto Star 2002). A few articles reported concerns about the impact of media discourse connecting the label of ‘criminal’ to people with FASD: “The stigma of FASD has grown worse in Winnipeg in the last few years since it was associated with a string of auto thefts by local teens” (Winnipeg Free Press 2011). In one example, a young man explicitly commented on media discourse and sought to distance himself from the criminal label and stereotype: “…[FASD is] not as scary as you see in the media: ‘These people are going to steal your car.’ They’re a very small minority of people with FASD… No one should label everyone with FASD as potential criminals or dupes eager to be recruited by gangs, he said” (Winnipeg Free Press 2011).
Socioeconomic Status
Some articles discussed how FASD is typically incorrectly thought to only affect people with lower socioeconomic status (SES), or how poverty can exacerbate the sources and impact of FASD: “‘Poverty does magnify health risks. If you’re poor, you have less access to nutrition and health care and likely more psychosocial stressors…. If it’s [FAS], it’s worse. But poverty doesn’t cause [FAS]. Alcohol causes it’” (Globe and Mail 2003). Several articles also discussed how FASD affects people in wealthier socioeconomic brackets too: “Yet the label [of FAS] is still pinned most often on the children of poor… women… Invisible are the middle-class mothers who drink during their pregnancies, whose problems with the bottle are shamefully concealed behind closed doors… the expectant women most likely to imbibe are educated, older and of higher income” (Globe and Mail 2003). Some other articles discussed how diagnoses might differ across SES and racial dimensions, as in the case of the following article from the Winnipeg Free Press (2011): “Experts such as Chudley say it’s likely doctors treating the troubled children of white, middle-class parents zero in on similar cognitive problems such as attention deficit hyperactivity disorder and never think about prenatal alcohol exposure”.
Discussion
Stigma surrounding FASD affects many stakeholders, including individuals with FASD and their birth mothers, among others (Bell et al. 2015). Armstrong (1998), in a seminal paper, outlined the history of the construction of the diagnosis, observing how the early medical literature suggested “both the woman who drinks during pregnancy and her child are beyond hope and destined to be societal problems”. Stigmatizing these groups could lead to difficult life trajectories for individuals with FASD (Bell et al. 2015) and blame, shame, or perhaps even criminalization for women who drink while pregnant (Armstrong 1998, 2003; Eggertson 2013; Hui, Angelotta, and Fisher 2017). Our analysis provides a first account of how FASD is presented in Canadian newspapers, which could contribute to stereotyped beliefs about both people with FASD and women who drink while pregnant. Through an analysis of articles published in ten top newspapers in Canada over the last 15 years, we identified eight themes related to social content (See Table 1). Across our results, we posit that the stereotype of ‘the villain’ dominated and connects to both key stakeholder groups[5]. We unpack this stereotype for both 1) people with FASD, for whom the ‘villain’ stereotype can be seen in the news coverage connecting them with criminal behaviour; and 2) women who drink while pregnant, whose ‘villainy’, while occasionally connected to disability discourse via discussion of substance abuse disorders, was most often built on the social expectations surrounding women and motherhood.
Stigma and People with FASD: The ‘villain’ stereotype
The most common disability stereotype we identified in Canadian FASD coverage was the villainous, immoral, or deviant disabled person. Twenty nine percent of our sample discussed a connection between FASD and criminal behaviour (See Table 1). This coverage did not always invoke stereotypes; in fact, some articles explicitly pushed back against the ‘criminal’ label, or raised complex questions about culpability. However, the frequency with which the topic was raised, and occasional implied biological essentialism, could still provide fodder for stereotyping. Interestingly, it appears that the framing of people with disabilities as ‘villains’ is not universal across Canadian media. Haller et al.’s (2012) sample overlapped with ours to an extent (though broader, focused on all kinds of disabilities), including seven of the same sources and one shared year of coverage. However, while the victim stereotype appeared in both samples, the villain stereotype was not discussed in theirs, highlighting its potential specificity in the case of FASD.
In some fictional representations of disability, we can find instructive archetypal and extreme examples of the villain stereotype. Peter Pan’s Captain Hook (Dahl 1993) and the Lion King’s ‘Scar’ (his difference is marked by his name) are examples of characters whose physical impairments or differences are viewed as possible sources or manifestations of their villainy. As Dahl (1993) suggests: “It has been a convention of all literature and art that physical deformity, chronic illness, or any visible defect symbolizes an evil and malevolent nature and monstrous behaviour”. Notably, roughly 10% of people with FASD have noticeable and characteristic facial differences – potential fodder for such tropes ( Andrew 2011). Similarly, fictional examples of intellectual disability and mental illness (e.g., Batman’s The Joker), both of which can be elements of an FASD diagnosis, frame disability as a key source of a character’s evil or unwittingly dangerous behaviour.
The specific case of mental illness is a useful analogue for better understanding some of the discourse surrounding FASD and criminal behaviour. Mental illness has been a key source of academic reflection on stereotypes and stigmatisation in both the news and entertainment media. While fictional examples can represent clear and extreme versions of stereotypes associated with disabilities, echoes of the same stereotypes can be seen in journalism (Babic et al. 2017). As a highly relevant and timely example, a common stereotype about mental illness and criminality focuses on mental illness as the cause of mass shootings, when causal factors and the commission of such crimes are far more complex (Metzl and MacLeish 2015). Indeed, beyond mental illness, Barnes (1992) notes that emphasizing “the connection between intellectual impairment and criminality are both common in the tabloids and the ‘quality’ papers”.
Although offenders with FASD in our sample were never explicitly described as ‘villains’, it is hard to escape the implication that criminal behaviour is somehow unavoidable for people with FASD. “Secondary disabilities” like criminal behaviour are sometimes presented or understood as essential features of FASD. For example, Dej (2011) points to how children with FASD are initially perceived as “innocent victims worthy of intervention”, until that perception shifts to an image of “undeserving and hopeless” criminals in adulthood. This hopelessness permeates our sample, connecting permanent brain damage to a lifetime of seemingly ineffective interventions and burdensome costs on Canadians (Aspler et al. Under Review). Similarly, Robert Henry (2013) explores a troubling iteration of the FASD-criminal stereotype in the form of media narratives about an “FASD-gang link in indigenous communities”.[6] At the same time, our sample included statements suggesting that the connection between FASD and criminal behaviour needs to be nuanced or reduced.
Culpability and policy approaches to FASD and criminal justice
Discussions about criminal culpability revolved around three distinct possible impairments: 1) a poor understanding of consequences; 2) a poor ability to reason about the rightness and wrongness of an action; or 3) no intention to harm, but issues with impulse control. However, there is a lack of clarity about what kind of “primary disabilities” may be relevant for understanding crime in the context of FASD. An understanding of FASD that accommodates difficulty understanding consequences could lead to conclusions about the effectiveness of jail as deterrence, as opposed to an understanding of FASD tied to intent, which might mean aiming for a charge of, for example, manslaughter over murder. Further research into the moral reasoning of individuals with FASD could help clarify this issue; however, heterogeneity of the diagnosis could mean all three challenges exist across the spectrum. These complex questions about FASD and criminal culpability still typically rely on the assumption that some biological feature of the disorder alone inevitably leads to criminal behaviour – rather than complex combinations of individual and social factors (e.g., foster care, impairment, police training).
Discussions about the relationship between FASD and criminal behavior must tread cautiously or risk cementing essentialist accounts of people with FASD as inherently criminal. For example, in the 2014 hearings for federal bill C-583, a bill to amend the criminal code to consider an FASD diagnosis as a mitigating factor in sentencing, some witnesses suggested that the bill could constitute discrimination: “…[this] is likely to further create associations between FASD and criminality which will only serve to further stigmatize this condition” (Standing Committee on Justice and Human Rights 2015). While better accommodating FASD in a criminal justice context should be a priority, and amending the criminal code could ultimately be a good solution, we must remain sensitive to concerns that our efforts to help people with FASD, through policy or otherwise, may perpetuate the stigma we seek to minimize.
People with FASD: villains and victims both
In our sample, 8% of the articles framed people with FASD as either victims of crimes or as more likely to become victims than other groups. Implicit in these and other discussions was a dual narrative, seen elsewhere in the FASD literature, which shifts the framing of individuals with FASD from sympathetic child or adolescent victims to hopeless adult villains (Dej 2011). The victim framing, though prevalent in the context of crime, also appeared in relation to women’s drinking behaviour. A similar media study about alcohol and pregnancy in the US found three dominant frames: 1) dangerous mothers, about women’s behaviour while pregnant (similar to the stereotype found in our analyses); 2) fetal wellness, which provided health advice; and 3) victimization, about the complex relationships between the identities of women who drink while pregnant and their children with FASD (Connolly-Ahern and Broadway 2008). In the case of the third theme, the children were seen as victims of their mothers, while those children as adults were seen as ‘villains’ as well – victimizing others, now as criminals with FASD.
Stigma, FASD, motherhood and villainy
Unlike coverage in the US, which mentioned women on trial or arrested for “fetal abuse” (Connolly-Ahern and Broadway 2008), we did not find reports of Canadian women who drank alcohol during pregnancy being arrested or receiving other forced interventions. Despite a few op-eds calling for harsh punishment[7], the interventions reported were mostly potential support programs for at-risk women. In fact, the Canadian media effectively communicated a number of nuanced counter-narratives, including how it is important for women to be able to receive support in non-judgemental environments, or that women typically do not drink while pregnant with the aim of harming their fetus.
However, in coverage about and interviews with adoptive or foster parents, mothers were most often the focus – even when their partners were described as supportive – in line with concerns about women being held more responsible for the wellbeing of their children. In one example, the parents are referred to as “Carol and her husband”, explicitly detaching the father from his fatherhood, seemingly shifting the entirety of parenthood onto the interviewed mother[8]. It is also interesting that none of the stories about fathers who themselves have FASD, though admittedly small in number, were framed negatively, while the examples about mothers with FASD were almost entirely negative. The stories about fathers involved overcoming issues like drug abuse, finding jobs, and achieving a stable family life. In contrast, the negative stories about mothers with FASD explored the perpetuation of cycles of alcohol abuse leading to children who themselves also have FASD. It is striking how the responsibilities of fathers, when mentioned at all, were rarely covered.
Furthermore, we can point to articles that described experiences of shame, and fear of judgement or punishment, to indicate that presenting information about FASD in certain ways can have a negative impact on some women. Under the socioeconomic status sub-code, nuanced concerns were raised about the problematic stereotyping of mothers of children with FASD (e.g., as poor, as indigenous); however, the pushback against these stereotypes contained in our sample simply expanded the label of ‘bad mother’ to encompass all women from all walks of life and rarely explored broader concerns about community responsibilities, intersectionality, or partner-inclusive or even partner-focused prevention messages.
Our results are therefore consistent with observations made by Armstrong (1998) that the responsibility for FASD often falls directly on the shoulders of women alone. In the 1970s and 1980s, when the diagnosis was first constructed, a “conservative political climate” likely contributed to centering the conversation about FASD on personal responsibility (Armstrong and Abel 2000). Although the diagnosis initially focused on the children of “chronic alcoholic women” alone (Jones et al. 1973), researchers and clinicians soon expanded the definition to suggest “that any drinking by any pregnant woman was dangerous” (Armstrong 1998) – a narrative we still see in individual-focused abstinence-based public health messages (Zizzo and Racine 2017). Armstrong (1998) points to early medical writing about “fetal alcohol syndrome” (FAS)[9] that frame women who drink while pregnant as having “clearly failed to fulfill their roles as nurturers”, even when trouble nurturing was connected to factors typically understood as outside of one’s control (e.g., disease, trauma). In many different ways, even in complex circumstances, women who drink while pregnant were and continue to be perceived as guilty for failing to protect their children. Armstrong (1998), perhaps controversially, ultimately suggested that “moral fervor powered the discovery of [FAS] as much as medical curiosity”.
These narratives of responsibility lend themselves to commonly described frames of the ‘dangerous’ or ‘bad’ mother (Connolly-Ahern and Broadway 2008; Lowe, Lee, and Yardley 2010). Although not directly related to the history of the villain disability stereotype, framing women as bad or dangerous mothers certainly connects them to some kind of villainy. These kinds of attitudes, at least in certain jurisdictions in the USA (Paltrow and Flavin 2013), can be connected to punitive policies aimed at pregnant women – which have led to arrests and even forced interventions (Drabble et al. 2014; Hui, Angelotta, and Fisher 2017; Racine et al. 2015). Although such measures have not made their way into Canada, where substance use is not illegal during pregnancy (Hui, Angelotta, and Fisher 2017), similar negative and stigmatising attitudes underlie some possible policy and healthcare approaches, as well as some media coverage in our sample. Concerns in Canadian newspapers remain focused on subtler messages about individual responsibility, but still without emphasizing the importance of community support, social circles, or the role of the woman’s partner. This will not necessarily lead to punishment, but it can certainly generate public blame and private shame for pregnant women in need of support.
Limitations
This study has several limitations. First, we only included articles where keywords were present in the headline or lead paragraph to ensure that FASD, or alcohol and pregnancy, were central to the stories we analyzed. This could have excluded additional articles about themes like crime, for example, if a suspect was only connected to FASD in a later paragraph. Second, in including only the top 10 English-language newspapers in Canada, our sample focused on stories from certain larger cities (i.e., Vancouver, Edmonton, Calgary, Winnipeg, Toronto, Ottawa, Montreal), while excluding coverage from other major parts of the country (i.e., The North, Saskatchewan, and Atlantic Canada). There might have also been some local coverage we missed from smaller papers, towns, or reserves in the provinces from which we did have representation.
Third, we tried to sample major French newspapers in Canada; however, Factiva began archiving Le Journal de Montréal and La Presse starting in 2011. While we do not know if these sources discussed FASD before 2011, no articles were found from 2011-2015. This could help explain differences in knowledge across Canada (based on Canadian surveys), since respondents from Quebec were less aware of FASD compared to other Canadians (Environics Research Group 2006). It may also be caused by differences in attitudes toward drinking in different regions of the country (April and Bourret 2004). More research is needed to understand such regional and cultural differences. In addition, three other included sources suffered from gaps in database coverage: 1) the Edmonton Journal from Feb 2002 – Dec 2003; 2) the Toronto Star for 2003; and 3) the Vancouver Province before Sep 2008. As a final note about sources, as of 2010, six of ten newspapers were owned by a single corporation (Postmedia), and, prior to this, at least five of ten were owned by Canwest (2000-2010). Postmedia ownership explains a large segment of the cross-posted duplicates included in this sample.
Conclusion
Our analysis of Canadian newspaper articles discussing the social dimensions of FASD identified eight key themes: 1) crime associated with FASD; 2) more support needed for FASD stakeholders; 3) awareness of FASD; 4) family composition of people with FASD; 5) funding for FASD; 6) FASD and Indigenous populations in Canada; 7) secondary disabilities associated with FASD; and 8) impact of the social world on FASD. We explored our results through the process of stereotyping and stigma as applied to two key stakeholder groups: 1) people with FASD; and 2) women who drink while pregnant. The literature on disability stereotypes, notably the stereotype of ‘the villain’ and to a lesser extent ‘the victim’, helped us to better understand Canadian coverage of FASD. The victim stereotype related in turn to stereotyped expectations of motherhood – as in, people with FASD are seen as victims of women who drink while pregnant. Not all of the coverage in our sample reflected these stereotypes; indeed, some articles sought to challenge them. Looking forward, the mechanisms of stigma at work in the context of FASD should be further explored as well as their implications for people with FASD and mothers of children with FASD. Otherwise, well-intended public awareness campaigns and media coverage risk fueling stigma against those people whose health and wellbeing they aim to promote.
Funding and Acknowledgements
This work has been supported by a grant from NeuroDevNet (ER), now known as Kids Brain Health Network (KBHN), as well as by training awards from McGill's Integrated Program in Neuroscience (JA), the Canadian Institutes of Health Research (JA), and the Fonds de recherche du Québec – Santé (JA and NZ). We have no conflicts of interest to declare. We would also like to thank members of the Pragmatic Health Ethics Research Unit, previously the Neuroethics Research Unit, for their invaluable feedback on the development of this project and on previous drafts of this manuscript.
References
- Abadir, Anna Maria, and Abel Ickowicz. 2016. "Fetal alcohol spectrum disorder: reconsidering blame." Canadian Medical Association Journal: CMAJ 188 (3):171-2.
- Andrew, Gail. 2011. "Diagnosis of FASD: An overview." In Fetal alcohol spectrum disorders: Management and policy perspectives of FASD, edited by Edward Riley, Sterling Clarren, Joanne Weinberg and Egon Jansson, 127-48. Weinheim, BW: Wiley-Blackwell.
- April, Nicole, and Amélie Bourret. "Status report on fetal alcohol syndrome in Québec." Institut nationale de santé du Québec. https://www.inspq.qc.ca/pdf/publications/365-FetalAlcoholSyndrome.pdf.
- Armstrong, Elizabeth. 1998. "Diagnosing moral disorder: The discovery and evolution of fetal alcohol syndrome." Soc Sci Med 47 (12):2025-42.
- ———. 2003. Conceiving risk, bearing responsibility: Fetal alcohol syndrome & the diagnosis of moral disorder: JHU Press.
- Armstrong, Elizabeth, and Ernest Abel. 2000. "Fetal alcohol syndrome: The origins of a moral panic." Alcohol and Alcoholism 35 (3):276-82.
- Aspler, John, Natalie Zizzo, Emily Bell, Nina Di Pietro, and Eric Racine. Under Review. "Stigmatisation, exaggeration, and contradiction: An analysis of scientific and clinical content in Canadian print media discourse about fetal alcohol spectrum disorder."
- Babic, Dragan, Romana Babic, Ivan Vasilj, and Esmina Avdibegovic. 2017. "Stigmatization of Mentally Ill Patients through Media." Psychiatria Danubina 29 (Suppl 5):885-9.
- Barnes, Colin. "Disabling Imagery and the Media: An Exploration of the Principles for Media Representations of Disabled People, the First in a Series of Reports." Ryburn Publishing. http://disability-studies.leeds.ac.uk/files/library/Barnes-disabling-imagery.pdf.
- Bell, Emily, Gail Andrew, Nina Di Pietro, Albert Chudley, James Reynolds, and Eric Racine. 2015. "It’s a shame! Stigma against fetal alcohol spectrum disorder: Examining the ethical implications for public health practices and policies." Public Health Ethics 9 (1):65-77.
- Carter, Carolyn. 1997. "Ladies don't: A historical perspective on attitudes toward alcoholic women." Affilia 12 (4):471-85.
- Chudley, Albert, Julianne Conry, Jocelynn Cook, Christine Loock, Ted Rosales, and Nicole LeBlanc. 2005. "Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis." Canadian Medical Association Journal: CMAJ 172 (5 Suppl):S1-21.
- Connolly-Ahern, Colleen, and S. Camille Broadway. 2008. "“To booze or not to booze?” Newspaper coverage of fetal alcohol spectrum disorders." Science Communication 29 (3):362-85.
- Cook, Jocelynn, Courtney Green, Christine Lilley, Sally Anderson, Mary Ellen Baldwin, Albert Chudley, Julianne Conry, et al. 2016. "Fetal alcohol spectrum disorder: A guideline for diagnosis across the lifespan." Canadian Medical Association Journal: CMAJ 188 (3):191-7.
- Corrigan, Patrick, Juana Lorena Lara, Binoy Biren Shah, Kathleen Mitchell, Diana Simmes, and Kenneth Jones. 2017. "The Public Stigma of Birth Mothers of Children with Fetal Alcohol Spectrum Disorders." Alcoholism: Clinical and Experimental Research 41 (6):1166-73.
- Dahl, Marilyn. 1993. "The role of the media in promoting images of disability - Disability as metaphor: The evil crip." Canadian Journal of Communication 18 (1).
- Daniels, Cynthia. 1993. At women's expense: State power and the politics of fetal rights. Cambridge, MA: Harvard University Press.
- Day, Louis. 2000. "Stereotypes in Media Communication." In Ethics in Media Communications: Cases and Controversies, 408-35. Belmont: Wadsworth Thomson Learning.
- Dej, Erin. 2011. "What once was sick is now bad: The shift from victim to deviant identity for those diagnosed with fetal alcohol spectrum disorder." Canadian Journal of Sociology/Cahiers canadiens de sociologie 36 (2):137-60.
- Devotta, Kimberly, Robert David Wilton, and Niko Yiannakoulias. 2013. "Representations of disability in the Canadian news media: A decade of change?" Disability and Rehabilitation 35 (22):1859-68.
- Di Pietro, Nina, and Judy Illes. 2014. "Disparities in Canadian indigenous health research on neurodevelopmental disorders." Journal of Developmental and Behavioral Pediatrics 35 (1):74-81.
- Drabble, Laurie, Sue Thomas, Lisa O'Connor, and Sarah Roberts. 2014. "State Responses to Alcohol Use and Pregnancy: Findings From the Alcohol Policy Information System (APIS)." Journal of Social Work Practice in the Addictions 14 (2):191-206.
- Eggertson, Laura. 2013. "Stigma a major barrier to treatment for pregnant women with addictions." Canadian Medical Association Journal: CMAJ 185 (18):1562.
- Eguiagaray, Ines, Brett Scholz, and Caterina Giorgi. 2016. "Sympathy, shame, and few solutions: News media portrayals of fetal alcohol spectrum disorders." Midwifery 40:49-54.
- Environics Research Group. "Alcohol use during pregnancy and awareness of fetal alcohol syndrome and fetal alcohol spectrum disorder: Results of a national survey." Health Canada. http://www.phac-aspc.gc.ca/publicat/fas-saf-natsurv-2006/index-eng.php.
- Ganong, Lawrence, and Marilyn Coleman. 1995. "The content of mother stereotypes." Sex Roles 32 (7):495-512.
- Golden, Janet. 2000. "“A tempest in a cocktail glass”: Mothers, alcohol, and television, 1977–1996." Journal of Health Politics, Policy and Law 25 (3):473-98.
- Haller, Beth, Marcia Rioux, Mihaela Dinca-Panaitescu, Andrew Laing, Jessica Vostermans, and Paula Hearn. 2012. "The place of news media analysis within Canadian disability studies." Canadian Journal of Disability Studies 1 (2):43-74.
- Henry, Robert. 2013. "Moving beyond the Simple: Addressing the “Misuse” of the FASD-Gang Link in Public Discourse." The Journal of Indigenous Wellbeing: Te Mauri - Pimatisiwin 11 (2):241.
- Holland, Kate, Kerry McCallum, and R Warwick Blood. "Conversations about alcohol and pregnancy." Foundation for Alcohol Research and Education. http://fare.org.au/2015/08/conversations-about-alcohol-and-pregnancy/.
- Hui, Katrina, Cara Angelotta, and Carl Fisher. 2017. "Criminalizing substance use in pregnancy: misplaced priorities." Addiction 112 (7):1123-5.
- Jones, Kenneth, David Smith, Christy Ulleland, and Ann Streissguth. 1973. "Pattern of malformation in offspring of chronic alcoholic mothers." Lancet 1 (7815):1267-71.
- Koren, Gideon, Irena Nulman, Albert Chudley, and Christine Loocke. 2003. "Fetal alcohol spectrum disorder." Canadian Medical Association Journal: CMAJ 169 (11):1181-5.
- Link, Bruce, and Jo Phelan. 2001. "Conceptualizing stigma." Annual review of Sociology 27 (1):363-85.
- Lowe, Pam, Ellie Lee, and Liz Yardley. 2010. "Under the influence? The construction of Foetal Alcohol Syndrome in UK newspapers." Sociological research online 15 (4):2.
- Macnamara, Jim. 2005. "Media content analysis: Its uses, benefits and best practice methodology." Asia Pacific Public Relations Journal 6 (1):1.
- McCallum, Kerry, and Kate Holland. 2017. "‘To drink or not to drink’: Media framing of evidence and debate about alcohol consumption in pregnancy." Critical Public Health:1-12.
- Metzl, Jonathan, and Kenneth MacLeish. 2015. "Mental illness, mass shootings, and the politics of American firearms." American Journal of Public Health 105 (2):240-9.
- Newspapers Canada. "2009 Daily Newspaper Circulation Report." Canadian Newspaper Association. https://nmc-mic.ca/about-newspapers/circulation/daily-newspapers/.
- Oliver, Mike. 1996. "Defining Impairment and Disability: Issues at stake " In Exploring the Divide: Illness and Disability, edited by Colin Barnes and Geoff Mercer, 29-54. Leeds: The Disability Press.
- Paltrow, Lynn, and Jeanne Flavin. 2013. "Arrests of and forced interventions on pregnant women in the United States, 1973-2005: implications for women's legal status and public health." Journal of Health Politics, Policy and Law 38 (2):299-343.
- Racine, Eric, Ofek Bar-Ilan, and Judy Illes. 2006. "Brain Imaging: A Decade of Coverage in the Print Media." Science Communication 28 (1):122-42.
- Racine, Eric, Emily Bell, Natalie Zizzo, and Courtney Green. 2015. "Public Discourse on the Biology of Alcohol Addiction: Implications for Stigma, Self-Control, Essentialism, and Coercive Policies in Pregnancy." Neuroethics:1-10.
- Salmon, Jenny. 2008. "Fetal alcohol spectrum disorder: New Zealand birth mothers' experiences." Can J Clin Pharmacol 15 (2):e191-213.
- Salmon, Jenny, and Stephen Buetow. 2012. "An exploration of the experiences and perspectives of New Zealanders with fetal alcohol spectrum disorder." J Popul Ther Clin Pharmacol 19 (1):e41-50.
- Stade, Brenda, Joseph Beyene, Kathryn Buller, Shannon Ross, Kayla Patterson, Bonnie Stevens, Michael Sgro, Wendy Ungar, William Watson, and Gideon Koren. 2011. "Feeling different: the experience of living with fetal alcohol spectrum disorder." J Popul Ther Clin Pharmacol 18 (3):e475-85.
- Standing Committee on Justice and Human Rights. "Study on the Subject Matter of Bill C-583, An Act to amend the Criminal Code (fetal alcohol spectrum disorder)." http://publications.gc.ca/site/eng/9.800881/publication.html.
- Streissguth, Ann, Helen Barr, Julia Kogan, and Fred Bookstein. "Understanding the occurrence of secondary disabilities in clients with fetal alcohol syndrome (FAS) and fetal alcohol effects (FAE)." https://archive.org/details/understandingocc00stre.
- Zizzo, Natalie, and Eric Racine. 2017. "Ethical challenges in FASD prevention: Scientific uncertainty, stigma, and respect for women's autonomy." Canadian Journal of Public Health 108 (4):e414-7.
-
The use of the term “disability” to refer to both biological impairments and their interactions with the social environment does not align well with disability studies conceptions of disability. For a detailed exploration of distinctions and relationships between ideas like disability and impairment, the latter of which the notion of “primary disabilities” likely more accurately reflects, see Mike Oliver’s chapter on the topic (1996). ↑
-
We can see in these descriptions a model of disability oriented more toward the individual or medical – one that emphasizes impairment as the primary (though not necessarily singular) cause of disability. There are also other potentially relevant factors, like childhood trauma or bad experiences in group home environments. ↑
-
However, this study presents a few methodological limitations. The categories of women (i.e., with mental illness, with substance abuse issues, who have been jailed for minor offences, and birth mothers of people with FASD) can overlap. In addition, the description of birth mothers seems more negative than descriptions of the other groups. ↑
-
More than one third of this sample (100/286 articles) came from The Winnipeg Free Press, which won a 2010 CIHR grant to cover FASD and its “causes, social costs, treatments, and prevention” [quote in sample]. Throughout 2010 and 2011, they published 18 and 30 articles respectively, accounting for just under 17% of the total sample (48/286 articles). Even without the CIHR award, they would still have had the most FASD coverage (52 articles, compared to 41 from the Edmonton Journal and 32 from the Calgary Herald). Of the rest of the articles, more than a third came from the other Western provinces (British Columbia and Alberta – no newspaper from Saskatchewan was included). In total, almost three quarters of the sample comes from these three Western provinces, with only 27% (77/286 articles) coming from Ontario, English Quebec news, or national papers like The Globe & Mail. ↑
-
Other, less common stereotypes included people with FASD framed as burdens on families or on Canadian society (see (Aspler et al. Under Review)), or as victims, the latter stereotype sometimes relating to the framing of mothers as villains – i.e., people with FASD were implicitly and explicitly framed as victims of their mother’s behaviour. ↑
-
The stereotypes connecting Indigenous peoples in Canada to FASD persist, although as we reported, our sample did include some positive pushback. These FASD stereotypes move through other harmful stereotypes – including those of the ‘drunk Indian’. For more on this topic, see Di Pietro and Illes (2014) as well as (Aspler et al. Under Review). ↑
-
In (Aspler et al. Under Review), one theme (treatment of FASD) included examples of how we should treat women who drank while pregnant. In an op-ed from the Calgary Herald (2005), one reader articulated an extreme position, suggesting that “these doped-up druggies should be sterilized after the second child…” ↑
-
Admittedly, Carol is an anonymized individual given a pseudonym for the article; however, the husband is not even given an anonymous identity outside of his relationship to Carol. ↑
-
At the time Armstrong published her first article, the term FASD did not yet exist. The spectrum as a medical diagnosis was still being constructed, so she refers mostly to the original term “fetal alcohol syndrome”. She does, however, highlight concerns about the diffusion and widening of symptoms and descriptions of FAS (1998). ↑