Using Technology to Enhance Services and Supports for Children and Youth with Disabilities and Medical Complexity and their Families in Canada: A Scoping Review
Utilisation des technologies pour améliorer les services et les ressources pour les enfants et les jeunes ayant un handicap et des problèmes médicaux complexes et leurs familles au Canada : un examen de la portée
Alison J Gerlach, PhD
Associate Professor [corresponding author]
School of Child & Youth Care
University of Victoria, Canada
alisongerlach [at] uvic [dot] ca
Amarens Matthiesen, PhD
Graduate Research Assistant
School of School of Child & Youth Care
University of Victoria, Canada
Kim Bulkeley, PhD
Senior Lecturer
Sydney School of Health Sciences
University of Sydney, Australia
Katie Gibbs
Youth Community Researcher
School of Child and Youth Care
Abstract
In Canada and internationally, the use of technology to enhance community-based health and developmental services and supports with children and youth has increased dramatically as a result of the COVID-19 pandemic. In the Canadian context, how technology-enabled supports and services have developed and can be integrated as a long-term option in addition to in-person services requires further examination. This scoping review maps out existing and emerging themes in Canadian research published on how different technology modalities are being used in home and community settings with children and youth with disabilities and medical complexity and their families. A literature search conducted across seven databases between 2011 and 2023 resulted in potentially relevant publications, of which 12 met the inclusion criteria. The findings provide insights into how various technologies are being used and combined in order to provide parenting training and coaching and timely access to assessments in a continuum of care without the burden of travel time and costs. Also, the potential of technology to create peer support networks both for parents and older youth with disabilities. These findings can inform funding bodies and community organizations serving this population in undertaking in depth and critical analyses of how technology can be further integrated into hybrid models of service delivery. Further research and actions are also needed to address issues of digital equity.
Résumé
Au Canada et dans le monde, l’utilisation des technologies pour améliorer les services et les ressources communautaires en matière de santé et de développement auprès des enfants et des jeunes a augmenté de façon spectaculaire en raison de la pandémie de COVID-19. La façon dont les ressources et les services technologiques se sont développés et peuvent être ajoutés dans les options à long terme en plus des services en personne nécessite un examen plus approfondi en contexte canadien. Cet examen de la portée cartographie les thèmes existants et émergents dans la recherche canadienne publiée sur la façon dont différentes modalités technologiques sont utilisées à domicile et dans la communauté auprès d’enfants et de jeunes ayant un handicap et des problèmes médicaux complexes et leurs familles. Une recherche documentaire menée dans sept bases de données entre 2011 et 2023 a abouti à des publications potentiellement pertinentes, dont douze répondaient aux critères d’inclusion. Les résultats donnent un aperçu de la manière dont diverses technologies sont utilisées ou combinées pour fournir de la formation et du coaching aux parents ainsi qu’un accès rapide aux évaluations dans un continuum de soins sans le fardeau associé au temps et aux frais de déplacement. En outre, les technologies ont le potentiel de créer des réseaux de soutien par les pairs pour les parents comme pour les jeunes ayant un handicap plus âgés. Ces résultats peuvent orienter les organismes de financement et les organismes communautaires desservant cette population souhaitant entreprendre des analyses approfondies et critiques de la façon dont les technologies peuvent être mieux intégrées au sein de modèles hybrides de prestation de services. De plus amples recherches et d’autres actions sont nécessaires pour résoudre les problèmes d’équité numérique.
Keywords: Telehealth, telerehabilitation digital literacy, digital equity, early intervention, northern, rural.
Introduction
Emerging international evidence points to the efficacy of technology in improving access to and continuity of care for children and youth with chronic and complex health conditions (Farmer & Muhlenbruck, 2001; Hines et al., 2019; Kronberg et al., 2021), speech and language delays (Coufal et al., 2018; Fairweather et al., 2016; Grogan-Johnson et al., 2011; Sutherland et al., 2021), hearing impairments (Behl et al., 2017; Constantinescu, 2012; First Nations Health Authority, 2015; Stredler-Brown, 2017) and different neurodevelopmental disorders[1] (NDDs) including fetal alcohol spectrum disorder (FASD) (Ens et al., 2010; Hanlon-Dearman et al., 2014) and autism (Alfuraydan et al., 2020; Boisvert et al., 2010; Ellison et al., 2021; Gibbs & Toth-Cohen, 2011; Johnsson & Bulkeley, 2021; Lerman et al., 2020; Meadan & Daczewitz, 2014; Ogourtsova et al., 2023; Vismara et al., 2012). Importantly, the use of technology as a mode of service delivery with this population does not typically replace in-person services as a ‘distinct or separate intervention’ but used in addition to some in-person services (Cason, 2014; Meadan & Daczewitz, 2014).
Historically in high-income countries such as Canada, various forms of communication and information technologies have been used to enhance access to child/youth health and developmental services and supports for families living in rural and remote areas (Banbury et al., 2014; Behl et al., 2017; Finak et al., 2022; Johnsson et al., 2019); being posited as a cost-effective way for improving equity of access (Campbell et al., 2020; Dew et al., 2013; Fairweather et al., 2016) and addressing provider shortages (Cole et al., 2019). The flexibility and responsivity of technologies can also fit easily into families’ lives; supporting a coaching approach[2] in naturalistic settings and building parental self-efficacy (Behl et al., 2017; Cole et al., 2019; Finak et al., 2022; Hines et al., 2019; Kronberg et al., 2021; McCarthy et al., 2022; Poole et al., 2022; Stredler-Brown, 2017; Vismara et al., 2012; Wallisch et al., 2019). In the context of Indigenous families in Canada, virtual services can allow for specialized services to be provided in supportive community and home settings where family members and local service providers are more readily available (Canada's Health Informatics Association, 2013; Eriks-Brophy et al., 2008; Hanlon-Dearman et al., 2014).
Factors influencing the uptake of technology, include provider acceptance and skills, organizational policies (Dew et al., 2013; Johnsson & Bulkeley, 2021; Joshi et al., 2021), and funding (Cole et al., 2019; Farmer & Muhlenbruck, 2001; Provenzi et al., 2020), digital literacy[3] and digital equity for both families and service providers (Campbell et al., 2020; Cole et al., 2019; Provenzi et al., 2020; Seelman & Hartman, 2009). Digital equity has been defined in Canada as “a state where people can readily and effectively access and use technology to participate in our society [and] is intricately bound to health equity” (Alliance for Healthier Communities, 2020)
In Canada and internationally, the COVID-19 pandemic galvanized a dramatic uptake in the use of technology to deliver a wide range of services and supports for children and youth with disabilities (Buzhardt & Meadan, 2022; Camden & Silva, 2021; Ellison et al., 2021; Ganesan et al., 2021; Johnsson & Bulkeley, 2021; Kronberg et al., 2021; Martin et al., 2020; Ogourtsova et al., 2023). In order to better understand how using technology has developed and can be further integrated as a long-term mode of service delivery with children and youth with disabilities and medical complexity in Canada - the authors of this paper undertook a scoping review of Canadian peer-reviewed literature published between 2011 and 2023. A scoping review was selected over a systematic review as a feasible method for capturing and summarizing the extant literature (Levac et al., 2010) on how technology with children and youth with disabilities and medical complexity and their parents has been used to provide health-and developmental-related supports, information and services in families’ homes and local communities.
This scoping review sought to provide an overview and analysis of the relevant literature rather than a critical appraisal of study designs, which is customary in a systematic review (Pham et al., 2014). This scoping review uses the United Nations definition of disability as including children and youth who have “long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others” (United Nations Convention on the Rights of Persons with Disabilities, 2006). We have included children with medical complexity in our scoping review because in addition to having complex health conditions, this population experience functional limitations and disabilities and high utilization of home- and community-based services (Dewan & Cohen, 2013). In this scoping review, ‘technology’ is inclusive of mobile phones, texting, emailing, direct messaging applications (such as Facebook and WhatsApp) and desk-top or mobile video conferencing platforms such as Skype, Zoom and Microsoft Teams, social media, and Apps. The primary question guiding this scoping review was: How is technology being used to provide health-and developmental-related supports, information and services for children and youth with disabilities and medical complexity in home and community settings in Canada?
Scoping Review Methodology
This scoping review was guided by a methodological framework developed by Arksey and O’Malley (2005) and ensuing advancements proposed by Levac et al. (2010).
Identifying Relevant Literature
The identification of relevant literature involved several key steps. In consultation with a research librarian at the University of Victoria, an initial set of known or ‘seed’ articles were first located during an exploratory search phase. These seed articles were analyzed by Matthiesen to harvest an initial set of keywords and subject headings as part of the search strategy development process. Following this exercise, the authors collaborated on a search strategy in which variations of terms related to; (a) population (e.g., children, infants, families, caregivers, parents), (b) technology use (e.g., virtual care delivery, digital technology, telerehabilitation, videoconferencing), and (c) location (e.g., Canada, Alberta, British Columbia, Ontario etc.) could be combined. On February 22, 2023, Matthiesen entered the search strings into seven electronic databases (PsycINFO, ERIC, Web of Science, Medline, CINAHL, Cochrane Controlled Trials Register and Scopus).
Study Selection
The imported the search results into Covidence Systematic Review Software - a web-based software platform that streamlines the organisation, (multi-user) screening and de-duplication of articles in systematic reviews (Veritas Health Innovation). Following the automatic removal of duplicates in Covidence, the first two authors independently screened all titles and abstracts of articles in line with the inclusion criteria depicted in Table 1.
| Inclusion Criteria | |
|---|---|
| Population | Children and youth aged 0-18 years with disabilities and/or medical complexity (e.g., cerebral palsy, spina bifida, autism and FASD) Parents of this population |
| Service Delivery | Uses technology in home and community settings to support child/youth health and development |
| Study | Peer reviewed research articles Research conducted in Canada Written in English language Published between 2011 and 2023 |
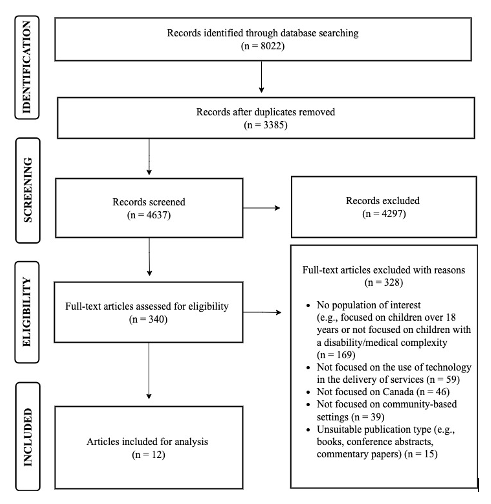
Matthiesen subsequently performed full text reviews of all articles that met one or more of the inclusion criteria. Articles that did not meet all inclusion criteria were excluded using custom-created reasons embedded in the Covidence software. As outlined in Figure 1, the initial keyword search resulted in a total of 8022 publications. After removing 3385 duplicates, Matthiesen undertook full-text reviews of 340 publications. When conflicts arose at the stage of abstract and/or full-text screening, these were discussed until the first two authors were able to reach final consensus on study inclusion. In addition, grey literature (e.g., news articles, government publications, conference proceedings) was excluded due to the lack of substantive content aligned with the inclusion criteria coupled with the sufficient volume of academic literature obtained. Consistent with the purpose of a scoping review, the date range (2011 – 2023) was selected to capture a broad array of literature, including the accelerated surge in the use of technology during the COVID-19 pandemic. Twelve articles were included for analysis.
Charting and Analyzing the Data
The first two authors collectively determined which variables to extract in order to answer the research question (Levac et al., 2010). These authors subsequently co-developed a codebook with the following extraction variables: research question/objective, study design, key study findings, location in Canada, disability/medical complexity, technology type(s) discussed and their facilitators/advantages and challenges/disadvantages, COVID-19 related information, and suggestions for future research. Using this codebook, the second author subsequently coded the data using web-based HyperRESEARCH software which facilitated the organization and coding of the corpus (Version 4.5.3, Researchware, Inc.). This software facilitated the data analysis process by uploading the included articles in the software, applying the extraction variables as codes to the data, and visualizing the prevalence of (sub)codes. The first two authors subsequently conducted a thematic analysis of the coded data, as a common method of data analysis in scoping reviews (Clarke & Braun, 2017; Finkelstein et al., 2021; Moola et al., 2020). The thematic analysis process also involved visual mapping of (sub)themes and multiple rounds of discussion between the first three authors.
Consulting with Community Stakeholders
As an optional component of a scoping review methodology (Levac et al., 2010), the lead author consulted with Brenda Lenahan, a parent community researcher partner and Katie Gibbs a youth community researcher to seek their input on a preliminary framing of the findings and their potential implications. Both community researchers provided feedback and were offered the opportunity to be recognized as co-authors.
Findings
The following Figure summarizes the search process and results.
A table in the Appendix summarizes the key characteristics of the research papers that met the inclusion criteria.
Themes in the Literature
Analysis of the 12 publications captured in this scoping review identified three themes in how technology has been developed and integrated in order to provide services, supports and education with children and youth with disabilities and medical complexity and their parents in Canada. A dominant theme in the literature was the use of technology to provide support for parents in their homes and local communities. This theme, and two smaller themes of using technology for timely assessments in a continuum of care and creating a sense of community for youth with disabilities, are discussed in the following section.
Supporting Parents in their Homes and Communities
Technology can clearly provide easier, flexible, timely and cost-effective access to information, services and supports that can be hard to access in-person; particularly for families in northern and remote areas of Canada (Burek et al., 2021; Hanlon-Dearman, et al., 2014; Hatton et al., 2019; Shire et al., 2021; Williams et al., 2022) and/or where services are in high demand, such as for young children with ASD (Shire et al., 2021; Wainer & Ingersoll, 2015). However, only a few studies underscored concerns about the lack of stable internet service in rural and remote areas and the constraints this placed on who participated in their research or could make use of technology-enabled services (Burek, et al., 2011; Hurtubise, et al., 2022).
Numerous studies examined how various technologies, and combinations of technologies, can support parents in raising children and youth with disabilities without the need to leave their home or community. In seeking to improve access to autism services, Wainer and Ingersoll (2015) evaluated the effectiveness of an internet-based program with remote coaching using videoconferencing to introduce five parents of young children (29 to 59 months old) with autism to ‘reciprocal imitation training’. Some parents described finding it challenging to maintain their children’s engagement in front of a video camera. However, overall parents in this study rated the video-based teaching tools most favorably and the majority of children in this study demonstrated changes in their spontaneous imitation skills within interactions with their parents. In response to the variability in parent engagement and learning observed in this study, the authors discussed the possibility of a “stepped-care service delivery model” to help address high demands for early intervention with young children with autism. The authors theorized that some parents may do well with a “low resource-intensive self-directed program” whereas others may benefit from more “intense support such as remote coaching” (p. 3887).
A 2021 study by Shire and colleagues aimed to address the challenges of access to regularly scheduled in-person autism services with families living in rural and remote communities in Newfoundland and Labrador, where travel time over challenging terrain is significant and expensive. The findings of this study with six families raising young children (2-9 years) with autism provides preliminary evidence supporting a shift to using videoconferencing, instead of in-person, to provide a ‘joint attention, symbolic play, engagement and regulation’ (JASPER) parent coaching intervention. At least one initial home visit was viewed as critical to building a relationship with the family, helping them set-up the necessary physical space and find toys that were developmentally appropriate. The researchers also noted that shifting to a remote environment, required more time to help parents with setting-up the environment for each coaching session and allowed the interventionist to focus on strategies rather than managing the environment and materials.
The benefits of ‘live coaching’ using videoconferencing to augment online, multimedia parenting information and education included increasing parents’ skills, knowledge and self-efficacy and child outcomes. Studies posited that the effectiveness of ‘live coaching’ was in part due to being able to see and connect with families in their own homes; gaining valuable insights into how to problem-solve and tailor strategies and resources for each family; taking into account siblings, parental values and home settings (Burek et al., 2021; Williams et al, 2022). However, Burek et al. (2021) also noted ‘logistical pressures’, including lack of space in families’ homes, children not participating, and ‘life interruptions’ that can limit the effectiveness of internet-based parenting interventions. The scheduling of coaching sessions was also recognized as a challenge particularly when both parents are working outside of the home (Shire et al., 2021).
In looking at improving accessibility to interventions and supports for children and families affected by FASD, Hundert et al., (2016) evaluated the content and usability of ‘an internet-based, distance intervention’ to provide parents of children between the ages of four and 12 with FASD with strategies for promoting their children’s development and improving parent child relationships. Online content was accompanied by weekly telephone sessions with a trained coach who tailored the program for each family’s situation and parents’ level of understanding. Participants (n=18), which included health care professionals with expertise in FASD and parents, rated the website as appealing and easy to use and identified concerns about the relevance and appropriateness of some of the content as it related to FASD.
Gaining parents’ feedback on website content was the focus of the study by Tan-MacNeill and colleagues (2020) which explored how 20 parents of children (aged four to ten years) with NDD perceived an ‘online, parent-implemented intervention’ for pediatric insomnia that was originally developed for ‘typically developing’ children. Multimedia content included five sessions on different sleep strategies. Parents in this study reported the intervention to be accessible, useful and feasible. Suggested modifications included having more specific content on sleep disorders and children with NDD. The authors of this study posited that the provision of accurate and ‘disease- or condition-specific’ online information can increase the efficacy of related virtual services (Tan-MacNeill et al., 2020).
More recent studies by both Burek et al., (2021) and Williams et al., (2022) examined the feasibility and acceptability of an adapted parent-child intervention program (I-InTERACT-North - Internet-based Interacting Together Every day: Recovery After Childhood TBI[4]) aimed at improving parenting skills and reducing emotional and behavioral difficulties in young children (aged 3-8 years) with neonatal brain injuries. The program involved seven self-guided modules on positive parenting and behavior management strategies. Completion of each one was followed by coaching via videoconferencing to review and contextualize the content for child and family specific circumstances. Handouts were created for families and emailed to them to support their learning of key components/skills. In the Burek et al., (2021) study, 19 of the 22 families enrolled completed the I-InTERACT-North program in an average of 10 weeks and reported high overall satisfaction and significant improvements in parenting confidence, parenting skill and child behavior. Some parents struggled with program adherence and suggested that having learning modules accessible on portable devices would help.
Positive outcomes were also noted in a slightly later study of the same I-InTERACT-North program undertaken by Williams et al., (2022) during the first year of the COVID-19 pandemic despite fewer referrals and lower completion rates (12 out of the 18 parents enrolled completed the program) attributed to parental stress, burnout and fatigue. This study during the height of the pandemic also provided insights that may be helpful in the long-term use of technology to support and coach parents. These included the importance of a coach spending time building strong relationships with families early in the training program, the use of motivational interviewing and enhancing program engagement by balancing flexibility with program structure and expectations. Reminder e-mails were also viewed as being essential for supporting scheduling and attendance. In response to the findings of this study, the research team reported a shift to delivering I-InTERACT-North in a ‘stepped-care model’ with ‘abbreviated coaching’ on basic parenting behavioral strategies and graduating to higher level strategies based on parental preference and need. Also, concerns about ‘Zoom fatigue’ as a result of parents and children spending many hours per day on this platform for work and school during the pandemic (Williams, et al., 2022) may also be a long-term limitation of videoconferencing, giving the ubiquitous use of this technology in families’ lives post-pandemic.
The sole use of videoconferencing to provide parents in northern and remote communities with education and supports was a feature of two studies (Hanlon-Dearman et al., 2014; Shire et al., 2021). In the research by Hanlon-Dearman and colleagues (2014) with 19 individuals from 16 families ‘affected by FASD’, parents valued how ‘telehealth’ using videoconferencing provided them with timely access to a diagnostic assessment and follow-up education and support, that would otherwise not be available without having to leave their home communities and travel long distances to urban-based services. This ‘telehealth’ program also created a safe and non-judgmental network in which parents could seek support, voice concerns and meet other parents experiencing similar challenges in caring for a child with FASD both within and beyond their own communities. Keeping families within their community and having family members and local community personnel take part in ‘telehealth’ was also viewed as particularly pertinent given the sensitivities involved with this diagnosis. Parents suggested that having babysitting services available would be helpful and that “receiving a brochure (or verbal explanation) outlining the telehealth process would be helpful and could decrease the intimidation some reported feeling prior to participating in a session” (Hanlon-Dearman et al., 2014, p. 5).
The ease of connectivity, peer support and information-sharing afforded by technology was clearly evident in the study by Kelly et al., 2022, which was the only one to explore the use of Facebook. This study explored how a closed, bilingual (English and French) Facebook group facilitated peer-to-peer (P2P) support for parents of children and youth with complex care needs in New Brunswick. The private designation of the Facebook group was an important consideration for attempting to protect group members’ confidentiality and creating a space conducive to the exchange of support. The 39 parent participants in this study reported using the group for navigational support for local programs, resources and activities and that having content focused on New Brunswick and a ‘patient navigator’ who contributed towards and moderated the group contributed towards their use of this group. Parents also noted the trustworthiness of information on various resources, programs and activities when it was based on parents’ lived experiences. Many of the parents reported using multiple PSP support groups for emotional purposes and information related to specific conditions. These findings highlight the potential of social media platforms like Facebook for supporting parents in navigating an often-overwhelming maze of information and services (Kelly et al., 2022).
The cost-saving benefits on travel for families and service providers was identified as a considerable benefit (Kelly et al., 2022; Shire et al., 2021). In addition, Hatton et al., (2019) reported that although a provincially funded telehealth-enabled screening program for infants’ hearing required costly installations of audiology equipment at various northern points-of-care, overall cost-savings were attributed to reduced travel times for service providers and families.
Accessing Timely Assessments in a Continuum of Care
Technology-enabled assessments with follow-up support were the focus of two studies. As outlined above, the findings by Hanlon-Dearman and colleagues (2014) reported not only on the use of ‘telehealth’ via videoconferencing for FASD assessment and diagnosis but also its capacity to provide this service in families’ home communities “in a continuous flow from intake to assessment to follow-up, with resulting enhanced patient care and increased community education and follow-up education” (p. 5). Conducting assessments with children living in remote areas was also a feature in the research by Hatton et al., (2019) that provided evidence on the accuracy, efficiency and scalability of a ‘telehealth-enabled auditory-brainstem response’ program in identifying infants with hearing loss. The authors of this study, echoing Hanlon-Dearman et al., (2014), pointed to the need for hearing assessments to be provided seamlessly in a “telehealth-enabled continuum of care for families with service access barriers that encompasses identification of hearing loss, counselling, technology and intervention services” for families across all geographical areas (p. 391)
The need to integrate technology-enabled services into a continuum with existing services was also underscored by stakeholders, including a small group of four parents, in the study by Hurtubise and colleagues (2022). This research informed a logic model for a new ‘primary care early intervention telerehabilitation service’ and identified factors that could influence its implementation. The proposed logic model integrated different services (coaching, P2P support etc.,) and delivery formats including videoconferencing, messaging and online forums and resources. Identified implementation factors included service providers’ attitudes and skills associated with ‘telerehabilitation interventions’ and their willingness to shift towards a hybrid model of in-person and virtual service delivery. Providing sustainable funding, access to technological supports, provision of training and education for those involved, financial and policy support, technology privacy and security standards were also viewed as key to supporting such a shift. The importance of adapting professional regulations, organizational policies and procedures to reflect this model were also identified as key to the sustainability of a hybrid model of service delivery (Hurtubise, et al., 2022).
Creating a Sense of Community with Youth
Two related studies looked at how an online forum for youth with cerebral palsy and spina bifida afforded a safe space to share information and foster interpersonal connections with peers and adult mentors with similar disabilities and lived experiences (Barnfather et al., 2011; Stewart et al., 2011). The earlier study by Stewart et al., (2011) involved a pilot online peer support program with 22 youth with cerebral palsy and spina bifida, who were 12-18 years old, had a grade 6 reading level and an IQ greater than 80. The program featured five young adult peer mentors with the same disabilities who met weekly online with the youth for 25 group sessions over six months. Technologies used included email, message boards and chat rooms integrated under the ‘Ability Online[5]’ interface. Topics included living independently, health concerns and building relationships. Youth participants reported a significant increase in sense of community with decreased loneliness and increased confidence.
The extent to which youth used this online peer support program was further examined in a study by Barnfather et al., (2011) which further concluded that a virtual environment was effective in ‘breaking down’ the barriers and vulnerability that youth with spina bifida or cerebral palsy may experience with in-person communications about their health conditions (Barnfather et al., 2011). However, some of the youth in this study expressed concerns about online cyber bullying and judgement and a desire for privacy and caution with online postings about their health. The authors suggested that this form of peer support may be most valuable when offered at “key points of stress such as transitions into new schooling environments” and that youth who are minimally impacted by their disability may not perceive the need for “disability-focused intervention” (p. 31). The authors also noted the need to consider accessibility issues and suggested that for youth with “more several physical disabilities, asynchronous chats may be more optimal as speed of response is less essential” (p. 31).
Discussion
The following section draws on the findings of this scoping review to underscore the promising possibilities afforded by technology within a hybrid model of service delivery for children and youth with disabilities and medical complexity who need low-barrier access to timely information, supports and services in their homes and local communities. Concerns related to digital equity and areas for further research are also raised.
The findings of this scoping review clearly demonstrate that the emerging Canadian evidence base provides encouraging evidence on the efficacy of using different technological modalities to enhance the provision of a range of home- and community-based supports, information and services for children and youth with disabilities and their parents. This evidence is well aligned with international research published before (Behl et al., 2017; Farmer & Muhlenbruck, 2001; Hines et al., 2019; Meadan & Daczewitz, 2014) and during the COVID-19 pandemic (Buzhardt & Meadan, 2022; Ellison et al., 2021; Gray et al., 2021; Johnsson & Bulkeley, 2021; Kronberg et al., 2021; Poole et al., 2022) and which continues to emerge as hybrid models of service delivery are further explored and integrated with in-person modes (Graham et al., 2023; Ogourtsova et al., 2023; Provenzi et al., 2020).
For families living in rural and northern parts of Canada who have stable internet service and technology in their homes, various technological modalities have a significant role to play in enhancing their timely access to information, services and supports that would otherwise not be available without extensive time, travel and expense (Burek et al., 2021; Hanlon-Dearman, et al., 2014; Hatton et al., 2019; Shire et al., 2021; Tan-MacNeill et al., 2020; Williams et al., 2022). This review highlights the value of hybrid service models that critically appraise and attend to the needs of individuals so that service responses that include technology are contextually tailored (Barnfather et al., 2011; Hundert, et al., 2016; Stewart et al., 2011; Tan-McNeill et al., 2020). As evident in the findings of this review, videoconferencing technology for coaching purposes has enhanced the accessibility to, and uptake of, parent training supports when asynchronous internet-based learning resources are combined with videoconferencing that allows for the tailoring of ‘live coaching’ so that the training can be more responsive to parent learning needs and family circumstances (Burek et al., 2021; Wainer & Ingersoll, 2015; Williams, et al., 2022).
Regardless of where families live, the combining of different technological modalities can also be effective in counteracting the potential isolation from individualized modes of service delivery, by fostering social support networks and a sense of community for parents (Hanlon-Dearman et al., 2014; Hundert et al., 2016; Kelly et al., 2022; Wainer & Ingersoll, 2015) and youth (Barnfather et al., 2011; Stewart et al., 2011). Evidence also points to the integration of different technologies in the provision of a continuum of ‘family-oriented services’ within a hybrid model (Hurtubise, et al., 2022). A hybrid model may also align well with a ‘stepped-care’ approach to service delivery’ that provides varying levels of support and care and allows for a larger number of families to be served by high-demand services, such as those for children with autism (Wainer & Ingersoll, 2015). Given that only one study in this scoping review focused on children with ‘complex care needs’ (Kelly et al., ) who tend to be high users of services indicates the need for further research on how technology can support service provision with this population in the Canadian context.
Importantly, organizations engaged in providing health- and developmental-related information, technology-assisted services and supports with this population require sustainable funding, technical infrastructure and supports and policies to address confidentiality and privacy concerns. Organizations also need the necessary resources for educating and mentoring professionals to effectively implement technology as an optional mode of delivering their services (Hanlon-Dearman et al., 2014; Hatton et al., 2019; Hurtubise et al., 2022).
The promises of the flexibility, cost-savings, and timely access afforded by technology also need to be carefully considered from an equity perspective as this option is only available to families who have access to affordable, stable and high-speed internet and the necessary technology in their homes or communities (Burek, et al., 2021; Wainer & Ingersoll, 2015; Williams et al., 2022). Despite being a wealthy country, there is a ‘digital divide’ in Canada between families who have access to technology and its benefits and those who do not (Canadian Internet Registration Authority, 2022; Gray et al., 2021). According to a 2021 report, while almost 91% of Canadian households had access to high-speed internet, only 59% of families in rural and remote areas and 42% of households on First Nations had the same access. As more services move ‘online’ there are serious concerns about inequitable access and urgent solutions are needed to address the urban-rural gap (Office of the Auditor General of Canada, 2023). If left unaddressed this ‘digital divide’ risks exacerbating current health and health care inequities (Gray et al., 2021).
Pertinent to addressing issues of digital equity, several studies identified the need to recruit ‘more diverse’ research participants in future research given that the diversity of the Canadian population is frequently not reflected in technology-enabled interventions (Burek et al., 2021; Hurtubise, et al., 2022). Moreover, to address the tendency for studies to have predominately female participants, Hanlon-Dearman et al., (2014), suggested that future studies explore potential gender differences in how parents engage with educational or support groups in videoconferencing-enabled programs. Further research centering the views of children of all ages with disabilities is also needed to ensure the careful use and adaptation of technology so that it is the ‘best fit’ to optimize participation. Moreover, there is a need for research in this field to engage with and clearly identify a greater diversity of children of all ages and parents including First Nations, Métis and Inuit views and experiences (Barnfather, et al., 2011; Hanlon-Dearman et al., 2014).
Limitations
Scoping reviews of literature aim to capture a breadth of evidence in a timely manner so that it can be used to inform practice and policy implications and are not intended to be exhaustive or evaluate the quality of the evidence. The parameters of this review did not include the use of technology by in-patient hospital- and tertiary-based settings, or in the mental health sector and which may be important to capture in future scoping reviews.
Conlusion
Virtual modes of service delivery were on the rise in Canada before the pandemic (Gray et al., 2021). Both in Canada and internationally, the pandemic stimulated a rapid shift in the use and acceptability of technology modalities and increased interest in retaining or further integrating technology into a long-term hybrid model of service delivery with children and youth with disabilities and medical complexity (Ellison et al., 2021; Gray et al., 2021; Johnsson & Bulkeley, 2021; Martin et al., 2020). This scoping review provides insights into how various technologies are being used and combined in order to provide parenting training and coaching and timely access to assessments in a continuum of care without the burden of travel time and costs. Also, the potential of technology to create peer support networks both for parents and older youth with disabilities. These findings can inform funding bodies and community organizations serving this population in undertaking in depth and critical analyses of how technology can be further integrated into hybrid models of service delivery. Further research and actions are also needed in Canada to address issues of digital equity.
Funding
We are extremely grateful to the Vancouver Foundation for a grant for the ‘Community Voices on Tapping into Tech’ study which funded this scoping review.
Endnotes
- ‘Neurodevelopmental disorders’ are a group of conditions with onset in the developmental period, including intellectual disabilities; communication disorders; autism spectrum disorder; attention-deficit/hyperactivity disorders and neurodevelopmental motor disorders (American Psychiatric Association, 2013).
- Coaching includes a range of strategies to support and strengthen parents’ ability to foster their child’s healthy growth and development. Strategies can include demonstration, joint problem-solving, guided practice, scaffolding, observation and feedback and reflection (Stewart, & Applequist, 2019).
- The Ministry of Education and Child Care in BC defines digital literacy as “the interest, attitude and ability of individuals to appropriately use digital technology and communication tools to access, manage, integrate, analyze and evaluate information, construct new knowledge, create and communicate with others” (https://www2.gov.bc.ca/gov/content/education-training/k-12/teach/resources-for-teachers/digital-literacy)
- I-InTERACT-North - Internet-based Interacting Together Every day: Recovery After Childhood TBI: https://i-interact.aboutkidshealth.ca/
- Ability Online is an online community for youth and young adults with disabilities or health challenges: https://newabilityonline.org/
References
- Alfuraydan, M., Croxall, J., Hurt, L., Kerr, M., & Brophy, S. (2020). Use of telehealth for facilitating the diagnostic assessment of autism spectrum disorder (ASD): A scoping review. PloS One. https://doi.org/10.1371/journal.pone.0236415
- Alliance for Healthier Communities. (2020). Digital equity call to action: Bridging the digital divide. https://www.allianceon.org/sites/default/files/14.6%20Digital%20Equity%20Strategy%20Call%20to%20Action%20Bridging%20the%20Digital%20Divide.pdf
- Arksey, H., & O’Malley, L. (2005). Scoping studies: Towards a methodological framework. International Journal of Social Research Methodology, 8, 19-32. https://doi.org/10.1080/1364557032000119616
- Banbury, A., Roots, A., & Nancarrow, S. (2014). Rapid review of applications of e-health and remote monitoring for rural residents. Australian Journal of Rural Health, 22, 211-222. https://doi.org/10.1111/ajr.12127
- Behl, D., Blaiser, K., Cook, G. A., Garrett, T. S., Callow-Heusser, C., Brooks, B. M., Dawson, P., Quigley, S., & White, K. R. (2017). A multisite study evaluating the benefits of early intervention via telepractice. Communication Sciences, 30(2), 147-161. https://doi.org/10.1097/IYC.000000000000090
- Boisvert, M., Lang, R., Andrianopoulos, M., & Boscardin, M. L. (2010). Telepractice in the assessment and treatment of individuals with autism spectrum disorders: A systematic review. Developmental Neurorehabilitation, 13(6), 423-432. https://doi.org/10.3109/17518423.2010.499889
- Buzhardt, J., & Meadan, H. (2022). Introduction to the special issue: A new era for remote early intervention and assessment. Journal of Early Intervention, 44(2), 103-109. https://doi.org/10.1177/10538151221094546
- Camden, C., & Silva, M. (2021). Pediatric telehealth: Opportunities created by the COVID-19 and suggestions to sustain its use to support families of children with disabilities. Physical & Occupational Therapy in Pediatrics, 41(1). https://doi.org/10.1080/01942638.2020.1825032
- Campbell, J., Theodoros, D., Hartley, N., Russell, T., & Gillespie, N. (2020). Implementation factors are neglected in research investigating telehealth delivery of allied health services to rural children: A scoping review. Journal of Telemedicine and Telecare, 26(10), 590-606. https://doi.org/10.1177/1357633X19856472
- Canada's Health Informatics Association. (2013). Canadian telehealth report: Based on the 2012 telehealth survey. Canada's Health Informatics Association. https://www.coachorg.com/en/communities/resources/TeleHealth-Public-FINAL-web-062713-secured.pdf
- Canadian Internet Registration Authority. (2022). Getting connected: Funders and digital equity in Canada. https://www.cira.ca/resources/community-investment-program/report/getting-connected-funders-and-digital-equity-canada#page1-2
- Cason, J. (2014). Telehealth: A rapidly developing service delivery model for occupational therapy. International Journal of Telerehabilitation 6(1), 29-36. https://doi.org/10.5195/ijt.2014.6148
- Cole, B., Pickard, K., & Stredler-Brown, A. (2019). Report on the use of telehealth in early intervention in Colorado: Strengths and challenges with telehealth as a service delivery method. International Journal of Telerehabilitation, 11(1), 33-40. https://doi.org/10.5195/ijt.2019.6273
- Constantinescu, G. (2012). Satisfaction with telemedicine for teaching listening and spoken language to children with hearing loss. Journal of Telemedicine and Telecare, 18(5), 267-272. https://doi.org/10.1258/jtt.2012.111208
- Coufal, K., Parham, D., Jakubowitz, M., Howell, C., & Reyes, J. (2018). Comparing Traditional Service Delivery and Telepractice for Speech Sound Production Using a Functional Outcome Measure. American Journal of Speech-Language Pathology, 27(1), 82-90. https://doi.org/10.1044/2017_ajslp-16-0070
- Dew, A., Bulkeley, K., Veitch, C., Bundy, A., Gallego, G., Lincoln, M., Brentnall, J., & Griffiths, S. (2013). Addressing the barriers to accessing therapy services in rural and remote areas. Disability and Rehabilitation, 35(18), 1564-1570. https://doi.org/10.3109/09638288.2012.720346
- Dewan, T., & Cohen, E. (2013). Children with medical complexity in Canada. Paediatrics & Child Health, 18(10), 518-522. https://doi.org/10.1093/pch/18.10.518
- Ellison, K. S., Guidry, J., Picou, P., Adenuga, P., & Davis III, T. E. (2021). Telehealth and autism prior to and in the age of the COVID-19: A systematic and critical review of the last decade. Clinicl Child and Family Psychology Review, 24, 599-630. https://doi.org/https://doi.org/10.1007/s10567-021-00358-0
- Ens, C., Hanlon-Dearman, A., Cox Millar, M., & Longstaffe, S. (2010). Using telehealth for assessment of fetal alcohol spectrum disorder: The experience of two Canadian rural and remote communities Telemedicine and e-Health 872-877. https://doi.org/10.1089/tmj.2010.0070
- Eriks-Brophy, A., Quittenbaum, J., Anderson, D., & Nelson, T. (2008). Part of the problem or part of the solution? Communication assessments of Aboriginal children residing in remote communities using videoconferencing. Clinical Linguistics & Phonetics, 22(8), 589-609. https://doi.org/10.1080/02699200802221737
- Fairweather, G. C., Lincoln, M., & Ramsden, R. (2016). Speech-language pathology teletherapy in rural and remote educational settings: Decreasing service inequities. Internattional Journal of Speech-Language Pathology, 18(6). https://doi.org/10.3109/17549507.2016.1143973
- Farmer, J. E., & Muhlenbruck, L. (2001). Telehealth for children with special health care needs: Promoting comprehensive systems of care. Clinical Pediatrics 40(2), 93-98.
- Finak, P., Hastings-Truelove, A., Fecica, A., & Batorowicz, B. (2022). Therapy services for children and youth living in rural areas of high-income countries: a scoping review. Disability and Rehabilitation, 1-23. https://doi.org/10.1080/09638288.2022.2074552
- First Nations Health Authority. (2015). Telehealth brings speech language therapy to a young girl in remote Hartley Bay. http://www.fnha.ca/about/news-and-events/news/telehealth-brings-speech-language-therapy-to-a-young-girl-in-remote-hartley-bay
- Ganesan, B., Fong, K. N. K., Meena, S. K., Prasad, P., & Tong, R. K. Y. (2021). Impact of COVID-19 pandemic lockdown on occupational therapy practice and use of telerehabilitation - A cross sectional study. European Review for Medical and Pharmacological Sciences, 25(9), 3614-3622. https://doi.org/10.26355/eurrev_202105_25845
- Gibbs, V., & Toth-Cohen, S. (2011). Family-centred occupational therapy and telerehabilitation for children with autism spectrum disorders. Occupational Therapy in Health Care, 25(4), 298-314. https://doi.org/10.3109/07380577.2011.606460
- Graham, F., Williman, J., Sutherland, L., & Wijninckx, M. (2023). Telehealth delivery of paediatric rehabilitation for children with neurodisability: A mixed methods realist evaluation of contexts, mechanisms and outcomes. Child: Care, Health and Development, 49(1), 156-169. https://doi.org/https://doi.org/10.1111/cch.13028
- Gray, C., Mason, J., & Loshak, H. (2021). An overview of direct-to-patient virtual visits in Canada. Canadian Journal of Health Technologies, 1(6). https://canjhealthtechnol.ca/index.php/cjht/article/view/eh0091
- Grogan-Johnson, S., Gabel, R. M., Taylor, J., Rowan, L. E., Alvares, R., & Schenker, J. (2011). A pilot exploration of speech sound disorder intervention delivered by telehealth to school-age children. Int J Telerehabil, 3(1), 31-42. https://doi.org/10.5195/ijt.2011.6064
- Hanlon-Dearman, A., Edwards, C., Schwab, D., Cox Millar, M., & Langstaffe, S. (2014). 'Giving voice': Evaluation of an integrated telehealth community care model by parents/guardians of children diagnosed with fetal alcohol spectrum disorder in Manitoba. Telemedicine and e-Health, 20(5), 478-484. https://doi.org/10.1089/tmj.2013.0161
- Hines, M., Bulkeley, K., Dudley, S., Cameron, S., & Lincoln, M. (2019). Delivering quality allied health services to children with complex disability via telepractice: Lessons learned from four case studies. Journal of Developmental and Behavioral Pediatrics, 31, 593-609. https://doi.org/0.1007/s10882-019-09662-8
- Johnsson, G., & Bulkeley, K. (2021). Practitioner and service user perspectives on the rapid shift to telehealth for individuals on the autism spectrum as a result of COVID-19. International Journal of Environmental and Public Health, 18. https://doi.org/10.3390/ijerph182211812
- Johnsson, G., Kerslake, R., & Crook, S. (2019). Delivering allied health services to regional and remote participants on the autism spectrum via video-conferencing technology: lessons learned. Rural Remote Health, 19(3), 5358. https://doi.org/10.22605/rrh5358
- Joshi, A., Paterson, N., Hinkley, T., & Joss, N. (2021). The use of telepractice in the family and relationship services sector. https://apo.org.au/sites/default/files/resource-files/2021-05/apo-nid312207.pdf
- Kronberg, J., Tierney, E., Wallisch, A., & Little, L. M. (2021). Early intervention service delivery via telehealth during COVID-19: A research-practice partnership. International Journal of Telerehabilitation, 13(1), 108. https://doi.org/https://doi.org/10.5195/ijt.2021.6363
- Lerman, D. C., O’Brien, M. J., Neely, L., Call, N. A., Tsami, L., Schieltz, K. M., Berg, W. K., Graber, J., Huang, P., Kopelman, T., & Cooper-Brown, L. J. (2020). Remote coaching of caregivers via telehealth: Challenges and potential solutions. Journal of Behavioral Education, 29, 195-221. https://doi.org/10.1007/x10864-020-09378-2
- Martin, J., McBride, T., Masterman, T., Pote, I., Mokhtar, N., Oprea, E., & Sorgenfrei, M. (2020). COVID-19 and early intervention: Evidence, challenges and risks relating to virtual and digital delivery. https://www.eif.org.uk/report/covid-19-and-early-intervention-evidence-challenges-and-risks-relating-to-virtual-and-digital-delivery
- McCarthy, M., Leigh, G., & Arthur-Kelly, M. (2022). Comparison of Participants' Behaviors During Telepractice and In-Person Family-Centered Early Intervention: An Exploratory Study. Infants & Young Children, 35(3), 222-247. https://doi.org/10.1097/iyc.0000000000000218
- Meadan, H., & Daczewitz, M. E. (2014). Internet-based intervention training for parents of young children with disabilities: A promising service-delivery model. Early Child Development and Care. https://doi.org/10.1080/03004430.2014.908866
- Office of the Auditor General of Canada. (2023). Connectivity in rural and remote areas: . https://www.oag-bvg.gc.ca/internet/docs/parl_oag_202303_02_e.pdf
- Ogourtsova, T., Boychuck, Z., O’Donnell, M., Ahmed, S., Osman, G., & Majnemer, A. (2023). Telerehabilitation for children and youth with developmental disabilities and their families: A systematic review. Physical & Occupational Therapy in Pediatrics, 43(2), 129-175. https://doi.org/10.1080/01942638.2022.2106468
- Pham, M. T., Rajić, A., Greig, J. D., Sargeant, J. M., Papadopoulos, A., & McEwen, S. A. (2014). A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res Synth Methods, 5(4), 371-385. https://doi.org/10.1002/jrsm.1123
- Poole, M. E., Fettig, A., McKee, R. A., & Gauvreau, A. N. (2022). Inside the virtual visit: Using tele-intervention to support families in early intervention. Young Exceptional Children, 25(1). https://doi.org/10.1177/1096250620948061
- Provenzi, L., Grumi, S., & Borgatti, R. (2020). Alone with the kids: Tele-medicine for children with special healthcare needs during COVID-19 emergency. Frontiers of Psychology, 11(2193). https://doi.org/https://doi.org/10.3389/fpsyg.2020.02193
- Seelman, K. D., & Hartman, L. M. (2009). Telerehabilitation: Policy issues and research tools. International Journal of Telerehabilitation, 1, 47-58. https://doi.org/10.5195/ijt.2009.6013
- Stredler-Brown, A. (2017). Examination of coaching behaviors used by providers when delivering early intervention via telehealth to families of children who are deaf or hard of hearing. Perspectives of the ASHA Special Interest Group SIG 9, 2(Part 1). https://doi.org/10.1044/persp2.SIG9.25
- Sutherland, R., Hodge, A., Chan, E., & Silove, N. (2021). Clinician experiences using standardised language assessments via telehealth. International Journal of Speech-Language Pathology, 23(6), 569-578. https://doi.org/10.1080/17549507.2021.1903079
- Tan-MacNeill, K. M., Smith, I. M., Weiss, S. K., Johnson, S. A., Chorney, J., E, C., Shea, S., Hanlon-Dearman, A., Brown, C. A., Godbout, R., Ipsiroglu, O., Reid, G. J., & Corkum, P. V. (2020). An eHealth insomnia intervention for children with neurodevelopmental disorders: Results of a usability study. Research in Developmental Disabilities, 98. https://doi.org/10.1016/j.ridd.2020.103573
- Veritas Health Innovation. Covidence systematic review software. www.covidence.org
- Vismara, L. A., Young, G. S., & Rogers, S. J. (2012). Telehealth for Expanding the Reach of Early Autism Training to Parents. Autism Research and Treatment, 2012, 121878. https://doi.org/10.1155/2012/121878
- Wallisch, A., Little, L., Pope, E., & Dunn, W. (2019). Parent perspectives on an occupational therapy telehealth intervention. International Journal of Telerehabilitation, 11(1). https://doi.org/10.5195/ijt.2019.6274
| Author(s) and Title of Paper | Location in Canada | Description of Technology & Use 6 | Population(s) | Methods | Key Findings |
|---|---|---|---|---|---|
| Barnfather et al., (2011) Computer-mediated support for adolescents with cerebral palsy or spina bifida |
Alberta | Online peer-support intervention via a website | 24 youth (aged 12-18 years) and peer mentors with cerebral palsy or spina bifida | Qualitative (as part of a larger mixed methods study) | • The online environment created a safe space to foster reciprocal interpersonal connections and appropriate social comparison. • Two-thirds of the participants viewed the computer-mediated support intervention as ‘fun’ • Factors influencing the perceived utility of the intervention included typing speed, cognitive skills and perceived need for additional support. |
| Burek et al. (2021) Transdiagnostic feasibility trial of internet-based parenting intervention to reduce child behavioural difficulties associated with congenital and neonatal neurodevelopmental risk: Introducing I-InTERACT-North |
Ontario | ‘Parenting skills training program’ using website(s) and coaching via Zoom video-conferencing | 22 families of children (ages 3-8 years) with neonatal and congental brain injuries | Mixed methods | • 19 families completed the program in an average of 10 weeks (range: 6-17weeks). • Parents reported high overall satisfaction with the program, including acceptability of both the online modules and the videoconference sessions. • Parenting confidence, parenting skill and child behaviour significantly improved over the course of the intervention. • Findings provide preliminary evidence for the feasibility, acceptability, and efficacy of I-InTERACT-North for parents of children with neonatal brain injury. |
| Hanlon-Dearman et al., (2014) ‘‘Giving Voice’’: Evaluation of an Integrated telehealth community care model by parents/guardians of children diagnosed with fetal alcohol spectrum disorder in Manitoba |
Manitoba | ‘Telehealth community-care model’ using videoconferencing (platform not specified) | 16 parents of children (age unspecified) with FASD | Qualitative | • Parents pleased with telehealth service for assessment, diagnosis, and/or follow-up support. • Parents appreciated the flexibility of telehealth, allowing them to remain in home communities connected to families and support systems. |
| Hatton et al. (2019) Telehealth-enabled auditory brainstem response (TH-ABR) testing for infants living in rural communities: the British Columbia Early Hearing Program experience |
British Columbia | ‘Telehealth-enabled auditory-brainstem response-programme using video-conferencing (Cisco MOVI/Jabber) and remote telemetry desktop software’ (name not specified) | 102 infants (mean age: 2.3 months) with hearing loss and 41 parents | Survey research | • The TH-ABR program was suitable, sustainable and scalable. After 29 TH-ABR events, the service was cost neutral. • Fifty infants were identified with hearing loss and TH-ABR accuracy and efficiency were comparable to face-to-face assessments. • Parent survey results indicated a high level of satisfaction with the TH-ABR experience. |
| Hundert et al., (2016) Usability testing of guided internet-based parent training for challenging behavior in children with fetal alcohol spectrum disorder |
Alberta, British Columbia, Manitoba, New Brunswick, North West Territories, Ontario, Saskatchewan, Yukon | ‘Internet-based, distance intervention’ accompanied by telephone sessions with a coach | 8 parents of children (4-12 years) and 10 service providers with expertise in FASD (inc. physicians, nurses, physiotherapists, occupational therapists) | Survey research | • Participants rated the website as appealing and relatively easy and fast to use. • Several usability problems were identified such as difficulty navigating between sections of content on the website, displaying too much content per page, and the relevance and appropriateness of the content as it related to FASD. |
| Hurtubise et al. (2022) Rethinking early intervention rehabilitation services for children with motor difficulties: Engaging stakeholders in the conceptualization of telerehabilitation primary care |
Unspecified Canadian province(s) | (Proposed) ‘Telerehabilitation intervention’ using videoconferencing (platform not specified) (or telephone if preferred), private messaging and an online forum | Focus groups conducted with 9 clinicians, 5 pediatric health care managers, and 2 technology consultants. Interviews conducted with 4 parents. | Participatory | • Participants supported the delivery of telerehabilitation services for children with mild motor difficulties. • Recommendations were voiced related to service relevance and sustainability, parent and community capacity building, and platform dependability, security, and support. • Identified factors influencing the implementation included consumer, provider, technological, systemic and contextual barriers and facilitators. |
| Kelly et al. (2022) Exploring the use of a Facebook-based support group for caregivers of children and youth with complex care needs: Qualitative descriptive study |
New Brunswick | ‘Web-based peer-to-peer support group’ using Facebook | 108 caregivers of children with complex care needs | Qualitative | • Five themes emerged from the interviews related to the use of a closed Facebook group and mediating factors of interactions between group members - resource for information, altruistic contribution, varying level of engagement, perceived barriers to and facilitators of group activity, and moderators as contributing members. |
| Shire et al. (2021) A technology-enabled adaptation of face-to-face caregiver-mediated JASPER intervention: Preliminary examination of video conferenced caregiver coaching |
Newfoundland and Labrador | ‘Telehealth’ using videoconferencing via Microsoft Teams and GoToMeeting software on personal devices including laptops and smart phones | 6 parents of children (ages 2-9 years) with autism | Multiple baseline, mixed methods | • JASPER (Joint Attention, Symbolic Play, Engagement, and Regulation) was adapted from traditional face-to-face caregiver coaching to using videoconferencing. • The results offer preliminary evidence of the effectiveness of real time video conference coaching for caregivers engaging their children with autism in play. |
| Stewart et al., (2011) Brief report: An online support intervention: Perceptions of adolescents with physical disabilities |
Alberta | ‘Online support intervention’ using e-mail, message boards, chat rooms under ‘Ability Online’ website (a free internet community for children with disabilities) | 22 youth (12-18 years) and 5 mentors with spina bifida or cerebral palsy | Mixed Methods | • Participants reported more contact with teens with disabilities, decreased loneliness, and increased social acceptance and confidence. • A significant increase in sense of community was reported from post-intervention to delayed post-intervention. |
| Tan-MacNeill et al., (2020) An eHealth insomnia intervention for children with neurodevelopmental disorders: Results of a usability study |
Unspecified Canadian province(s) | ‘eHealth/online intervention’ using a website | 20 parents of children (4–10 years) with NDD and insomnia | Survey research | • Participants reported the intervention to be usable, useful, acceptable, and feasible. • Several modifications were suggested to make the intervention more appropriate and acceptable for use with children with NDD. |
| Wainer, et al., (2015) Increasing access to an ASD imitation intervention via a telehealth parent training program |
Ontario | ‘(Hybrid) telehealth’ program using a website | 5 children (29-59 months) with autism and their parent(s) | Mixed methods | • Parents improved in their use of the intervention techniques and their children demonstrated concurrent increases in spontaneous imitation skills. • Parents also indicated that the intervention and telehealth service delivery model were acceptable, useable, and effective. • Results suggest that this hybrid telehealth program has the potential to increase access to autism services. |
| Williams et al. (2022) Pandemic perils and promise: Implementation of a virtual parenting intervention during COVID-19 among children with early neurological conditions |
Ontario | ‘Parenting skills training program’ using website(s) and coaching via Zoom video-conferencing | 22 families of children (ages 3-9 years) with a neurological condition (e.g., neonatal stroke, epilepsy, autism, preterm birth) | Mixed methods | • Parents reported strong therapeutic alliance and programme acceptability with barriers due to competing time demands. • Therapists reported high acceptability but perceived parental burnout. • Parenting confidence and child behavior improved following the intervention. • Results demonstrate the programme’s value to families during the pandemic, while underscoring unique participation barriers. |