ABLEISM ENTRENCHED: Inside the Pedagogical Politics of Canada’s MAiD Curriculum
Catherine Frazee OC, D.Litt., LLD. (Hon.)
Professor Emerita
Toronto Metropolitan University
School of Disability Studies
cfrazee [at] web [dot] net
Abstract
This article seeks to illuminate the chasm that exists between the promise of a stringent, humane and equitable MAiD regime and the actual realities of MAiD for non-dying persons [known as Track 2, or “T2 MAiD”]. It arises from efforts and observations during the course of a two-year engagement with the Canadian Association of MAiD Assessors and Providers [CAMAP], primarily as a member of a working group tasked with development of one of the course modules for a national program of MAiD practitioner training. During that time, the author learned much about the ideological culture within which T2 MAiD is practised, the considerations that play out in clinical MAiD assessments and the life circumstances of disabled persons who are deemed ‘eligible’ for T2 MAiD. Her good faith efforts of two years revealed to her that the only way that high-ranking practitioners and advocates in positions of authority can justify MAiD Track 2 practice is if it is shorn of any critical reflection about how dominant ableist assumptions have historically shaped and continue to shape the lives, realities, suffering and death of disabled persons. Such reflection, the author concludes, is antithetical to MAiD Track 2. As the suffering of social and material deprivation, stigma, trauma and toxic insecurity afflict more and more disabled Canadians, modern medicine has failed to evolve to meet the challenge of tending to our pain. Entrusted instead with a straightforward, deadly, but sure-fire “cure” for complex human suffering, the institutions of medical authority – self-governing regulatory colleges and influential practitioners who established and now lead CAMAP – embraced the law and made it their own. Along the way, they shed any sense of obligation to understand the problem of human suffering more deeply, to engage in critical ethical reflection, or to respond with the time-consuming and painstaking work of life-affirming care.
Keywords: Medical Assistance in Dying; Ableism; Track 2 MAiD; Ethics
In March of 2021, a consequential amendment to Canada’s medical assistance in dying (MAiD) law[1] came into force despite near-universal opposition from the country’s disability rights sector[2]. The legalization of Track 2 MaiD — permitting assisted death for persons with disabilities whose deaths are not reasonably foreseeable — was heralded by lawmakers and many commentators as a triumph of autonomy and compassion. For disability rights advocates, however, it marked something far more chilling: the entrenchment of a legal regime that applies exclusively to people with disabling medical conditions and that reconfigures death as a remedy for lives deemed intolerable. This critical disconnect between the aspirations of disability justice advocates and the will of Parliament has given disabled Canadians reason to pause. For the past five years, scholars, activists, and community leaders have reflected on how MaiD expansion moved forward despite vigorous opposition, strategized how best to mitigate its harms, and sought to make intelligible what is at stake when disability becomes the threshold for lawful death. The Canadian Journal of Disability Studies has been centrally located in that work of reflection, witnessing, debate and mobilization.
A substantial body of disability studies scholarship now situates Canada’s MAiD regime within longer histories of exclusion, abandonment, and eugenic reasoning. Valentina Capurri traces how contemporary policy debates reproduce older discourses of social worth and inadmissibility; Heidi Janz argues that systemic ableism permeates end-of-life decision-making in ways that render disabled lives precarious; Nancy Hansen documents the disappearance of disability from MaiD discourse even as disabled bodies remain its primary subjects; Michele Hutyra analyzes how inaccessible life is normalized while assisted death is endorsed; Hilary Pearson interrogates the alignment of MaiD with state health governance, tracing how discourses of population health and system efficiency obscure the differential valuation of disabled lives. Gabrielle Peters, writing from within disability justice activism, sharpens this critique by naming the sovereign power at stake: the authority to designate certain populations as expendable and to cultivate what she calls a “killable class.”[3] From multiple vantage points, these scholars converge on a shared insight: assisted death cannot be understood apart from the material conditions, social hierarchies, and policy failures that structure disabled people’s lives. Autonomy discourse, when detached from structural analysis, risks legitimating abandonment rather than remedying it.
Of course, disability scholarship does not speak with a single voice on assisted dying. Alexandre Baril and others have urged careful attention to the intersecting logics of ableism and sanism, complicating any attempt to reduce MaiD debates to a simple opposition between disability rights and autonomy.[4] Scholars may diverge on what justice ultimately demands of an assisted dying regime. Yet there is broad convergence on the necessity of structural clarity: any ethical engagement with MaiD must confront the power relations that shape how suffering is produced, interpreted, and legitimated.
All of this work builds upon foundational disability studies analyses of ableism as more than discrimination or prejudice. In her foundational work, Fiona Campbell described ableism as the production of “abledness” as the normative ideal of the human, against which disabled lives are measured and diminished.[5] Talila Lewis situates ableism within interlocking systems of colonialism, racism, capitalism, and eugenics, underscoring its material and epistemic force.[6] Shelley Tremain’s analysis of medical governance demonstrates how disability is constituted through institutional practices that classify, regulate, and manage populations under the guise of neutral expertise.[7] Jasbir Puar’s account of debility and differential valuations of life, together with Nirmala Erevelles’ work on disposable bodies, illuminate how states distribute care, neglect, and premature death along axes of disability, race, and economic precarity.[8] Allison Kafer’s political-relational account of disability further reminds us that autonomy is never solitary but always shaped by collective arrangements of care, dependency, and futurity.[9] By these accounts, ableism is not simply an attitude; it is a structuring logic that shapes whose lives are supported, whose suffering is normalized, and whose deaths are rendered intelligible.
The judicial logic that brought MAiD into legislative possibility rested In significant measure on trust in the medical profession. In Carter v. Canada (Attorney General), Justice Lynn Smith concluded that the risks of harm in a physician-assisted dying regime could be “greatly minimized,” provided appropriate safeguards were in place. She emphasized that the effectiveness of those safeguards would depend in part on “the skills and commitment of the physicians who are responsible for working within them” and on meaningful monitoring and enforcement.[10] Canadian physicians, she observed, were already experienced in assessing competence, voluntariness, and non-ambivalence in end-of-life decision-making, and were capable of applying “the very highest level” of scrutiny to assisted dying decisions.[11] This reasoning — later affirmed by the Supreme Court of Canada — rested on a high degree of confidence in professional judgment, ethical integrity, and institutional accountability. The durability of Canada’s MaiD regime depends, in no small measure, on that trust.
Yet well before MaiD’s expansion, disability scholars had cautioned that medicine’s self-understanding as neutral and benevolent masked deeply entrenched ableist assumptions. For example, writing in 2019, Heidi Janz described ableism as “the undiagnosed malady afflicting medicine,” noting that it frequently presents as “common sense” within clinical discourse — shaping judgments about quality of life, suffering, and appropriate intervention while appearing ethically neutral.[12] The concern, then, is not that MaiD introduced ableism into medical practice, but that it provides a new legal site in which longstanding patterns could operate with lethal consequence.
This article enters this now-mature and ongoing conversation in critical disability studies from a distinct vantage point, interrogating how the judicial and legislative trust vested in medicine is translated into MaiD practice, and what is lost in that translation. It examines how questions about vulnerability, ableism, and the social production of suffering are received, reframed, and ultimately contained within the pedagogical apparatus that trains MaiD practitioners. Its analysis is grounded in my two-year engagement with the Canadian Association of MaiD Assessors and Providers (CAMAP) as a contributor to the development of its practitioner training curriculum. What began as an invitation to help shape a humane and inclusive approach to capacity and vulnerability assessment evolved into a sobering encounter with the dominant culture of medical authority when challenged to face its own embedded ableism. Rather than fostering reflection or inviting discomfort, the CAMAP curriculum functions to reinforce the status quo: a MaiD regime in which social suffering is medicalized, disability stigma and disadvantage are framed as irremediable, and the moral burden of euthanasia is neutralized by procedural detachment. The result is a polished, pedagogy-proof system — one effectively sealed off from educational content that might prompt critical thinking, ethical inquiry, or transformative learning. Instead, the CAMAP MaiD curriculum transmits procedural knowledge without moral reflection, training assessors to look away from the structural and psychosocial dimensions of suffering and to dismiss critical perspectives as ideological. What follows is a firsthand account of how this architecture was built, how dissenting views were suppressed, and how the concept of disability was strategically evacuated of political meaning. It reveals a systematic sanitizing of clinical discourse, a refusal to grapple with the eugenic legacy of medicine, and an overriding resistance to ethical complexity — culminating in a regime that forecloses meaningful anti-ableist reform.
This article does not aim to generalize about the broader culture of medicine, though its observations may resonate beyond MaiD. It remains narrowly focused on the specific institutional and ideological architecture that CAMAP has constructed to legitimate and operationalize MaiD in general, and Track 2 MaiD in particular.
Diversity Managed: A Token Overture and a Controlled Narrative
My involvement with CAMAP began in 2021, when separate invitations were extended to participate in the development of two course modules: one introductory, the other focused on assessing capacity, vulnerability, and mental health. The first invitation, issued by CAMAP’s then-president, Dr. Stefanie Green, requested a short video script representing “the perspective of the disability community.” Dr. Green specified a two-minute maximum, apologizing for the time restriction but framing the invitation as an effort to acknowledge “legitimate concerns” about MAiD.
Even at this early stage, the constraints were telling. The request framed the disability perspective not as a vital analytic framework or body of rights-based knowledge, but as a minority viewpoint to be squeezed into a brief aside — which would ultimately be positioned after clinicians had been guided through a carefully curated chronology portraying MAiD’s expansion as progressive, inevitable, and ethically uncontested. There would be no serious effort to grapple with the complexity of disability critique, nor any recognition that this critique has been grounded in decades of resistance to medical paternalism, structural inequality, and eugenic ideology. Instead, CAMAP appeared content to treat disability concerns as a checkbox item in a pedagogical sequence aimed at positioning clinicians as unassailable agents of enlightened social progress, rather than subjects of valid ethical scrutiny.
Ultimately, it seemed most prudent to decline the invitation. The tight format, combined with CAMAP’s editorial oversight, offered insufficient latitude for meaningful intervention. Indeed, the final version of the introductory module does not include a video as Dr. Green had described, nor does it engage with disability as a site of structural critique. A single slide (see Figure 1) lists “Disabilities” [sic] as one of “various perspectives” on MAiD, reducing the disability position to two generic concerns about devaluation and coercion. These concerns are then immediately countered with a rebuttal also attributed to the “disabilities” perspective, thus effectively positioning disability rights opposition as fractured and therefore non-authoritative. The slide’s structure reinforces a false equivalence between a collective, rights-based critique and an individual account of preference, placing both on the same analytic plane and obscuring the distinction between structural justice claims and competing personal viewpoints.
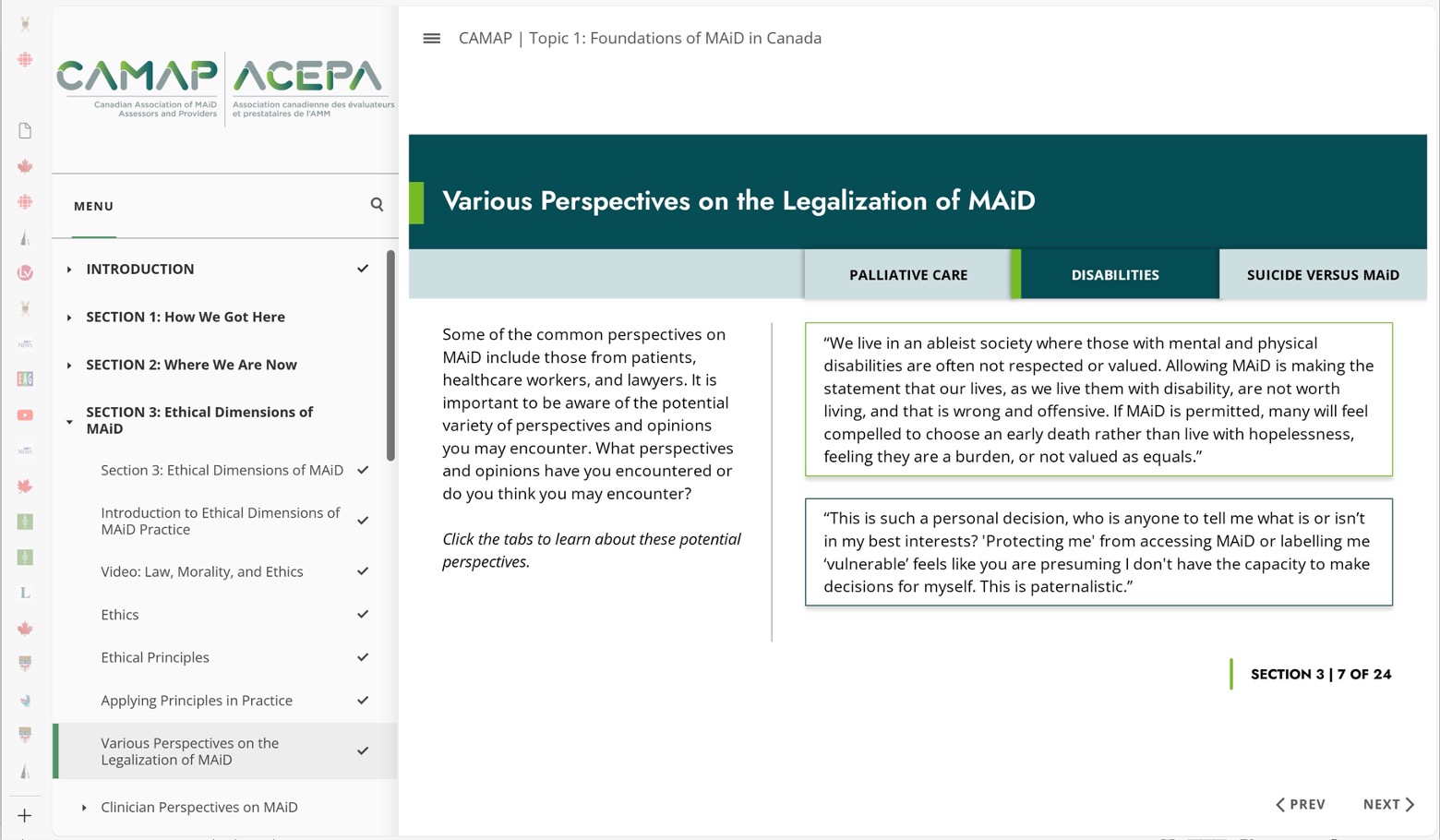
Such flattening is not merely rhetorical. By constructing disability as one “perspective” among many, rather than as a socially constructed category that, especially in intersection with poverty and/or culturally marginalized identities, is uniquely and disproportionately targeted by Track 2 MAiD — CAMAP’s curriculum systematically erases the foundational reasons why it is overwhelmingly opposed by disability rights defenders. The introductory module reduces a long-standing record of protest, advocacy, and critical scholarship to a pairing of contradictory slogans and soundbites that are easily brushed aside. In doing so, it ensures that MAiD practitioners can absorb “awareness” of disability without being burdened by its implications. This is not simply a matter of rhetorical simplification; it is an unserious and tokenistic treatment of a body of knowledge and experience that is anything but simplistic.[14] By reducing “the disabilities perspective” to a pair of interchangeable slogans, CAMAP’s slide erases precisely the structural analysis that gives the disability critique its force.
Cordial Containment: Curriculum Working Group 4
A more sustained engagement began when I joined the working group responsible for developing CAMAP’s module on assessing capacity, vulnerability, and mental health[15] — referred to initially as the ACUMEN module. The group comprised five physicians (all MAiD providers), one ethicist, and myself as its sole lay participant — and the only consistent voice advancing a disability rights critique of Track 2 MaiD. Despite assurances that diverse perspectives would be welcomed, what unfolded was a pattern of cordial engagement followed by quiet erasure, with a disability rights perspective holding little sway in shaping the direction or eventual outcome of the work.
In early meetings, physicians spoke candidly about the cases they had assessed —some of which involved patients with stable disabilities, unaddressed psychosocial suffering, or plainly inadequate supports. One member noted matter-of-factly that some practitioners “do a lot of MaiD very hastily,” without fully considering vulnerability. Another expressed alarm that experienced providers lacked the capacity to hold ethical complexity in life-and-death decisions. Yet these reflections were rarely pursued further. The dominant framework remained focused on capacity, consent, and minimal thresholds for legal compliance — even when patient distress stemmed from complex, non-medical realities such as loneliness, unresolved trauma, poverty, or housing insecurity.
There was a marked absence of ethical discomfort in the working group’s treatment of cases where ableist injury appeared to underlie requests for MaiD; death was largely accepted as a lawful and therefore appropriate outcome. In one poignant case, a young disabled man was granted Track 2 MaiD after expressing despair at the prospect of never having a romantic relationship or a loving family. His request was supported by his mother, who was openly resentful of having been left without support to raise a disabled child. In another case, a homeless 19-year-old disabled man in hiding from a dangerously abusive family died by Track 2 MaiD after a formally coherent but ethically blinkered assessment process. In the view of his assessors, the case affirmed the primacy of patient autonomy: the young man was “level-headed and articulate”, and his cerebral palsy met the legal threshold of an irremediable condition. Under this narrow frame, there was no obligation to question the material deprivations or psychosocial trauma driving his despair.
Accounts like these, presented with clinical detachment by working group practitioners, resonate very differently among those of us situated within the human rights and critical disability sector, where such stories are recognized as deeply troubling indicators of structural failure. That failure is not incidental. As Gabrielle Peters has argued, MaiD discourse proceeds as if individuals were socially unencumbered actors — “unconstrained by their social or financial situation, unimpacted by the culture, economy, laws, or politics of their era.”[16] She describes this flattened account of agency as “astroturf autonomy”: a cultivated fiction of independence that renders deprivation, abuse, and exclusion invisible at the moment a request for death is assessed. Within such a frame, the structural production of despair disappears from view, and a young man’s despair can be treated as a coherent personal value rather than as the foreseeable consequence of abandonment. What is read as autonomy is, in fact, autonomy shaped — and in crucial respects foreclosed — by policy and power. But within the CAMAP working group, cases such as these generated little sense of ethical or professional urgency.
What these deaths revealed was not just the personal agony of ableist injury, but the MaiD regime’s inability — or unwillingness — to distinguish between suffering arising from the medical symptoms of a disabling condition, and suffering caused by systemic exclusion, cultural revulsion, and internalized stigma. For many practitioners, the distinction was irrelevant: the patient had capacity, the request was voluntary, and the death was lawful. The curriculum was being constructed to train assessors not to think critically about the logic of MaiD practice, but to implement it efficiently.
Robin’s Case: Reifying Ableism Through Simulation
As our work progressed, a fictional case study was introduced into our Working Group 4 module. Although I later learned that the scripted video described in the following paragraphs was ultimately not included in the final curriculum, the way it was framed, discussed and defended within the working group is nevertheless emblematic of a deeper collusion with the structural and psychosocial forces of ableism that would be reproduced throughout Canada’s MAiD curriculum.
“Robin,” a 40-year-old woman and former nurse, had become quadriplegic after a fall. She was presented as well-spoken, rational, and emotionally stable — but in profound emotional distress arising from her loss of independence, inability to resume her career, feelings of burdensomeness, and distress around requiring toileting assistance. While fictional, the case drew directly from clinical encounters shared by members of the working group. Notably, the case study framed Robin’s anguish as arising from conditions of her now-disabled life that conflicted with her deeply held personal values. This characterization proved highly problematic, as it diverted critical attention away from discussion of the possible roles of employment discrimination, inadequate support arrangements, incomplete rehabilitational adjustment, and the psychic toll of internalized ableism.
As originally scripted and subsequently produced in video format, the case narrative unfolded across three staged assessment meetings. Initially, Robin’s distress was palpable. She described being unable to hug her children, feeling like “a burden,” and finding her reliance on intimate personal care to be intolerable. Although her assessors offered counseling and support and Robin eventually emerged from her depression and despair, she ultimately reaffirmed her desire to die by Track 2 MAiD, declaring:
I realize now that it is better for them [her children] to be with their own mommy rather than someone else; no one can replace me completely. But I cannot live like this. I have tried to adjust the best way I can, and I know myself, and that being unable to function at the high level I functioned before is not a life I can stand. I also cannot get used to needing help on the toilet, by strangers. I know this isn’t a decision everyone would make, but these are my values.…. I still want MAID.[17]
When invited to review the draft script, I responded with a detailed critique. The scripting of Robin’s experience was suffused with ableist tropes — dependency as indignity, care reliance as humiliation, altered embodiment as diminished personhood. Rather than probing the roots of these beliefs, the script appeared to validate them. Robin’s despair was tied to her personal values, rather than being understood as a response shaped by ableist beliefs about dependence, bodily difference and worth. The case study seemed to validate despair as the natural outcome of acquired impairment and in so doing, reinforced for learners the idea that any expression of disability-linked distress, if expressed coherently, would be sufficient justification for state-sanctioned death.
Missing from the script were obvious questions: Could Robin’s despair be mitigated through environmental modifications, personalized disability supports, or professional reintegration? Could her aversion to toileting assistance be recognized not as a fixed value, but instead as an expression of internalized social stigma — one that could shift over time, or perhaps through anti-ableist counselling?[18] And ultimately: Must autonomy require uncritical acceptance of suffering, or might it demand active engagement with the sources of that suffering?
This critique was shared with the working group and with two senior members of the CAMAP curriculum oversight body. Only one respondent, along with the working group chair, acknowledged its ethical force. The rest, including members of the Canadian MAiD Curriculum Development Committee (CMCDC), responded by reasserting Robin’s eligibility and capacity. Her account of humiliation was accepted at face value. Several physicians recounted similar, MAiD-eligible, cases from their own practice, suggesting that the case was “realistic.” One observed that regardless of assessment rigour, patients could “learn to game the system” in advocating for Track 2 MAiD. Another pointedly insisted that assessors must not impose their “personal approaches to life”. In that response, the dominant cultural ideal of independent function was held as neutral, while a moral compass calibrated to disability experience was recast as idiosyncratic and merely personal.
Notably, none of these responses addressed the concern that Robin’s suffering was driven by internalized ableism — by values that cast dependence as indignity and disabled life as unendurable. My critique was effectively reinterpreted as threatening to undermine autonomy — an evaluation that functioned to delegitimize my interrogation of the social forces animating Robin’s despair. This logic, wholly embraced by CAMAP and embedded in its curriculum, positions MAiD practitioners as arbiters of formal eligibility, rather than as moral agents compelled to examine the structural conditions behind MAiD requests. Eligibility is settled once the legal thresholds of capacity and consent are met – regardless of what gives rise to the desire for death – so long as the request is clinically valid and competently expressed.
This position became clearer as members of the working group prepared materials to guide discussion of Robin’s case. In passages that appeared to anticipate and contain objections, facilitators were prompted to ask: “If Robin is the product of an ableist society, do we expect her to outrun society’s influences because we want that of her, or do we at some point allow her to be a product of her society?” A similar line of reasoning queried whether Robin’s convictions might simply be “consistent with the belief system of Western culture in which she lives, and whether we would therefore stop everyone from accessing MAID who is a product of their culture.” Whatever their provisional status, such reflections reveal a deeper orientation in CAMAP’s approach: one that aligns with rather than interrogates the ableist norms shaping patients’ perceptions of suffering.
But ableism, like racism, sexism, colonialism, or any other ideology of subjugation, is not a benign or culturally neutral “belief system” that clinicians are obliged to respect as difference. It is a system of power that organizes material conditions, constrains opportunity, and penetrates self-understanding.[19] It erodes belonging, normalizes diminished expectations, and trains both individuals and institutions to accept injustice as inevitable. Its effects are cumulative and pervasive: not only on disabled people whose lives are directly circumscribed, but on the broader culture’s understanding of what is just, fair, and worthy of protection. To treat such norms as culturally coherent expressions of patient identity is to naturalize injustice itself.
As Heidi Janz has warned[20] , medical ableism is most insidious when it masquerades as “common sense,” denying its own rhetoricity and presenting deficit-based assumptions about disabled life as neutral clinical judgment. Within such a milieu, suffering and disability become quietly conflated, and the prospect of death can be embraced as value-free without ever naming the hierarchy of human worth that underpins it.
In the name of respecting autonomy, this stance colludes with oppression—affirming despair as rational and culturally situated rather than recognizing it as shaped by forces that demand resistance. The clinician’s role is not to acquiesce in the face of internalized denigration, but to discern when suffering reflects structural harm and to refuse to translate that harm into eligibility for death. Rather than risk complicating an ethically streamlined practice, the curriculum trains practitioners to leave its ableist premises undisturbed.
Ultimately, the uncritical embrace of Robin’s case as pedagogically sound would become emblematic of how anti-ableist critique was received — and ultimately stripped of consequence —throughout the curriculum development process.
Erasure in Plain Sight: How a Curriculum Made Ableism Untouchable
To their credit, decision-makers at CAMAP and the CMCDC ultimately elected to include definitions of ableism and anti-ableism in the final course glossary. The definition of ableism, in particular, acknowledged the quiet subjugation of disabled states that lies at the heart of ableist worldviews:
Practices, policies, attitudes, and behaviours that reflect a presumption that the default human state is non-disabled and that disability in any of its forms is a diminished human state.[21]
This inclusion marked a modest but symbolically important step: an acknowledgement that ableism is real and at least relevant to MAiD assessment. But the above framing that appeared in the final module[22] represents a truncated version of the definition I had crafted and submitted during the working group’s development process. That earlier version had read:
Practices, policies, attitudes, and behaviours that reflect a presumption that the default human state is non-disabled and that disability in any of its forms is a diminished human state. Such practices and behaviours naturalize injustice, often rendering it invisible. They are generally rooted in imbalances of social power that are so pervasive as to be unrecognized.[23]
That the final version reproduces the first sentence verbatim but excludes the rest is telling. What was removed were not incidental elaborations but core insights: that ableism operates by naturalizing injustice, by elevating the norms of non-disabled life as both natural and ideal, and by concealing the power imbalances that shape how suffering and deprivation are understood, whether they are rendered actionable, and what form that action ultimately takes. For any conscientious MaiD practitioner, these dynamics are not peripheral — they are foundational. To omit them is to reduce ableism to a matter of mere interpersonal bias, rather than exposing its role in sustaining clinical norms that equate dependency with indignity, or disability with diminished value.
Likewise, the definition of anti-ableism was edited down to its most inert form. My original version had described it as:
A conscious commitment to grapple with the uncomfortable truth of how pervasively ableism is embedded in our values and behaviours, combined with demonstrated efforts to undertake the learning, deep reflection, and self-correction required to break free of ableism’s influence.[24]
However, in the final glossary, the phrase ends abruptly after the first clause – at “behaviours” – thus retaining the notion of discomfort, but stripping away any reference to ethical growth, behavioural change, or systemic transformation.
These editorial decisions did more than soften the glossary. They signaled a larger pedagogical strategy — one that allowed the curriculum to gesture toward systemic injustice without requiring practitioners to reckon with their own entanglement in it. By retaining only the least disruptive language, the curriculum offered the appearance of critical engagement while neutralizing its substance. The result was a version of ableism that could be acknowledged in passing, but never traced to how it shapes clinician behaviour or patient outcomes.
This broader refusal to name or locate responsibility extended well beyond the glossary. As detailed earlier, the curriculum’s treatment of Robin’s case was framed by a view that clinicians should defer to patients’ suffering as an expression of their cultural ethos — even when that context was pervasively shaped by ableist norms. The suggestion that physicians should not expect patients to “outrun” the effects of the ableist society in which they live was paired with an equally troubling suggestion: that to question such values would be to impose our own. Rather than confronting the ideological substrate of the patient's despair, practitioners were encouraged to regard it as natural, legitimate, and culturally situated — beyond critique and certainly beyond the scope of their professional responsibility. In this way, the curriculum did not merely fail to teach anti-ableist practice. It actively reassured practitioners that no such responsibility existed.
Curriculum Undone: Resistance, Retrenchment and Resignation
One of the clearest indications of institutional closing of ranks in the curriculum development process emerged around a proposed set of slides I had designed to prompt discussion about the relevance of ableism to Canadian MAiD practice. Among these was a single slide — reproduced in Figure 2 — that invited learners to reflect on the historical role of physicians in Canada’s eugenic past, and to consider how that legacy might inform an anti-ableist perspective in present-day MAiD assessment. Measured in both tone and structure, the slide acknowledged the good faith of past practitioners while locating their actions within the historical norms of their time. Even so, it marked a rare and necessary attempt to place medical authority in dialogue with its historical entanglements and the habits of thought they continue to sustain.
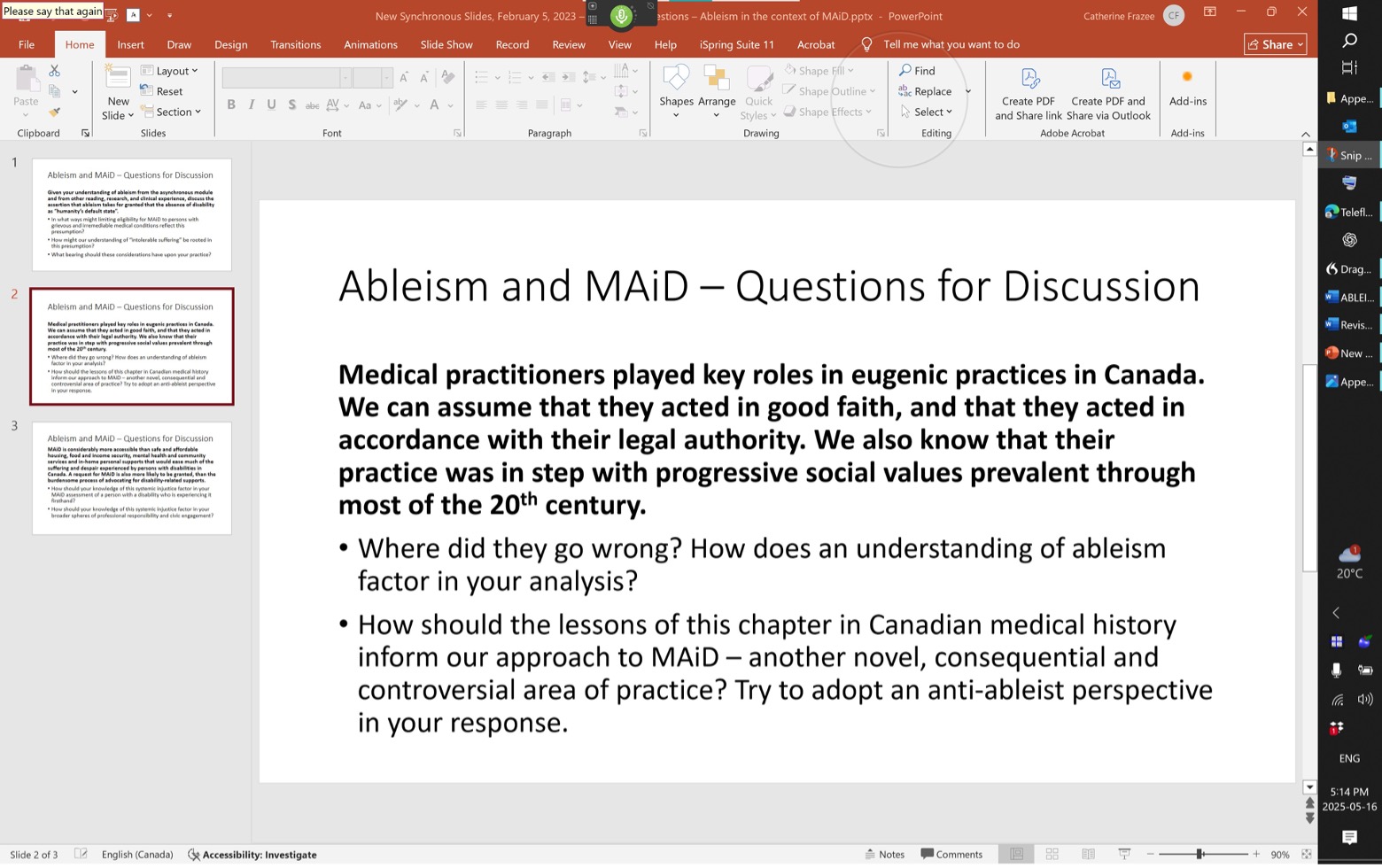
Despite its tempered tone, the slide triggered immediate unease among several working group members. Objections focused not on the discussion questions themselves but on the slide’s core factual premise — that medical practitioners had played a central role in implementing eugenic policies. One clinician warned that referencing eugenics might unfairly “stigmatize” physicians. Another objection was that doctors had merely enacted decisions made elsewhere in the system, and that it was inappropriate to single them out. It was argued that any specific reference to medical roles in eugenics should be removed. The objection was not to the historical facts themselves — none were disputed — but to the discomfort they might create for contemporary practitioners.
In response to this resistance, I revised the slide, offering a more succinct and open-ended prompt that removed any interpretive framing and simply asked: “How is the history of medical eugenics and its intertwining with ableist values and beliefs relevant for today’s MAiD practitioners?” This version — designed to allow facilitators and learners to approach the topic on their own terms — was included in the next draft of the module. But it, too, encountered strong pushback during review by senior CAMAP officials and members of the CMCDC. Reviewers described the slide as “not written in a way our learners will respect or accept”, and warned that it might “divert the discussion very quickly from the aim of the module.” One reviewer noted that “many presenters would not be comfortable addressing those issues.” The most pointed objection declared: “Ok, I have a problem with this.... To be frank, the slide and the facilitator's notes read like they were written by anti-track 2 advocates. Please rethink / redo this slide.” Though the revised slide had made no claims and posed no challenge to the legitimacy of MAiD, its very presence was seen as oppositional — too risky to retain. The intensity of the reaction it provoked stood in sharp contrast to the measured tone of the question itself, revealing just how threatening even a modest invitation to historical reflection could become within the confines of this pedagogical regime.
As the draft module advanced, resistance hardened. The CMCDC ultimately ordered that all reference to the eugenic era be removed entirely. As one senior figure in the discussion put it, “You do not feed the bad wolf.” Another warned that “opponents of MAiD” might seize upon such language. Despite clarification that the question was intended to promote historical literacy, not condemnation, the verdict was final: the word “eugenics” would not appear anywhere in the curriculum. A similar fate met a benign and factually accurate statement that “every person who meets the criteria for a grievous and irremediable medical condition can be considered to be a person with a disability.” Though designed to help situate MAiD within an anti-ableist pedagogical frame, this sentence was flagged as fraught with “political implications”, and summarily excised.
These interventions were not isolated incidents. They reflected a broader unwillingness to allow the curriculum to explore how systems of power — legal, medical, and cultural — shape both suffering and MAiD eligibility. Nowhere was this more apparent than in the evolving treatment of the concept of vulnerability. At the outset, the module had taken vulnerability as its central organizing concept. A detailed flowchart — originally developed to structure the entire module — had outlined a stepwise framework for integrating a focus on psychosocial vulnerability into MAiD assessment. Anchored at the module’s entry point, it instructed assessors to identify, explore, and take seriously the full range of social and structural conditions that may compromise autonomy. This process diagram was intended not only to guide practitioner reasoning, but to operationalize vulnerability as a foundational concern. Its eventual removal signaled a deliberate shift away from ethical reflection and toward a proceduralist framework in which capacity and consent were paramount, and vulnerability was relevant only if it interfered with the satisfaction of minimal legal criteria. This narrowing of purpose positioned MAiD assessors not as clinicians or moral agents, but as technicians of the law — functionaries tasked with applying eligibility criteria rather than exercising professional judgment.
With this shift, the curriculum lost the conceptual architecture that might have invited practitioners to interrogate how structural harm distorts patient decision-making or renders a MAiD death – particularly a Track 2 MAiD death – ethically questionable. What remained was a curriculum that taught procedural neutrality while deflecting moral engagement. Practitioners were trained to verify cognitive capacity and document voluntariness, but not to examine how suffering might have been rooted in abandonment, systemic inequality, or internalized oppression. The culture of MAiD, as reproduced in this training, made no space for discerning whether a patient was seeking death because of their disability, or because of how disabled lives are systematically rendered unlivable through processes of sustained deprivation and devaluation.[26] These distinctions — crucial in a regime where the outcome is death — were left unnamed and unexamined.
Taken together, these revisions stripped the module of any meaningful reckoning with the social and political forces that animate MAiD requests — not only in Track 2, but across the full spectrum of MAiD practice. Even in cases where death is reasonably foreseeable, case reports have shown how poverty, isolation, and structural vulnerability can play a decisive role in shaping a patient’s desire to die[27]. Under Track 2, where the patient is not dying and the ethical stakes are heightened, these forces become even more consequential. Yet rather than equipping practitioners to recognize and respond to such influences with nuance and care, the curriculum groomed them to adhere to a procedural façade of compliance — rehearsing eligibility criteria while leaving unexamined how structural inequality and cultural bias shape life-and-death decisions.[28] In doing so, it displaced the very qualities — judgment, reflection, and responsibility — that Canada’s MAiD legislation, in its own preamble[29], identifies as essential to a regime grounded in dignity, autonomy, and protection for vulnerable persons.
What was lost in this reframing was not simply emphasis, but analytic integrity. The Criminal Code requires that a person’s suffering be caused by their grievous and irremediable medical condition.[30] Yet the curriculum’s narrowing of vulnerability effectively collapsed the distinction between suffering that arises from a medical condition and suffering that is rooted in, or exacerbated by, social and cultural deprivation. Once vulnerability was repositioned as background context rather than as an interpretive lens, assessors were no longer invited to differentiate among the possible sources of suffering or to weigh their relative causal significance. If capacity was intact and consent coherently expressed, the assessment could proceed without sustained inquiry into whether the desire for death reflected medical decline or the cumulative effects of stigma, isolation, and abandonment.
Neither the law nor its associated regulations offer guidance on how clinicians are to assess causation in cases where medical decline and structural deprivation are intertwined[31]. While the law requires that suffering be caused by a grievous and irremediable medical condition, it does not specify how assessors are to distinguish between suffering attributable to pathology and suffering compounded — or even primarily produced — by poverty, inadequate supports, housing insecurity, or social exclusion.[32] Nor does Canada’s MAiD regime provide for independent, case-by-case oversight of these determinations. Compliance is largely monitored retrospectively and in aggregate, leaving significant interpretive authority in the hands of individual practitioners.[33] As Isabel Grant has observed, although Track 2 includes additional procedural safeguards, “eager providers have learned how to circumvent many of those safeguards”[34], underscoring the extent to which interpretive latitude shapes outcomes in practice. In this context, the curriculum’s retreat from a robust engagement with vulnerability does not merely reflect pedagogical preference; it effectively consolidates discretionary power at precisely the point where structural harms are most difficult to disentangle from medical decline.
This shift mirrored broader cultural assumptions about disability and suffering — assumptions extensively critiqued within disability studies scholarship. Scholars have argued that ableism does not merely misrecognize disability; it structures the material and affective conditions under which disabled lives are rendered precarious, devalued, or “better off dead.”[35] In this light, vulnerability cannot be treated as descriptive background. It is a product of policy, economics, and culture, and it shapes how individuals come to interpret their own distress and prospects. By permitting vulnerability to be acknowledged without consequence, the curriculum preserved existing assessment habits and shielded practitioners from confronting whether a request for MAiD might be the endpoint of cumulative structural harm rather than the expression of an irremediable medical condition. The distinctions that had once been central to the module’s design — between medical causation and social production of despair — were left formally visible but functionally inert.[36]
Curriculum Consolidation: A Regime Beyond Reform
What emerged from the CAMAP curriculum development process was not simply a flawed training module. It was a clear articulation of how Canada’s Track 2 MAiD regime understands — and refuses to understand — disability, vulnerability, and suffering. The final product of CAMAP’s intervention would be a pedagogical apparatus engineered to exclude systemic critique, suppress moral dissent, and reframe social abandonment as private pain. The curriculum would train assessors not in ethical discernment, but in ideological compliance.
At the core of this system is an epistemic sleight of hand. MaiD practitioners are taught that patient suffering must be accepted as self-interpreting and unassailable—so long as it is articulated with clinical coherence. They are not trained to examine what produces that suffering: whether it stems from structural exclusion, is intensified by ableist norms, or might be addressed through social or relational intervention. As long as patients meet the legal threshold of capacity and voluntariness, their reasons need not be questioned.[37] In fact, to question those reasons — especially if they implicate social or cultural oppression — is treated as an affront to autonomy.
This logic is not incidental. It is the defining logic of Canada’s Track 2 MaiD regime. And it is, at its core, ableist. It presumes that disabled people’s lives are not just harder, but plausibly unlivable — and that such conclusions can be mobilized by individual medical practitioners with no meaningful legal, ethical or peer review. It treats suffering linked to disablement as sufficiently ruinous to justify an exemption from the Criminal Code’s prohibition on homicide, and to invert the constitutional guarantees of equal protection and benefit of the law. It accepts demoralization born of deprivation, isolation, and structural neglect as medical phenomena, and authorizes the permanent erasure of those who suffer “too much,” without examining what that suffering is made of. It is a regime that answers social injury with death, and calls it medical care.
As Peters has insisted, MaiD is not plainly the recognition of a private “right to die”. Rather, MaiD law confers upon the state and licensed clinicians a new authority to administer death to a legally defined class of citizens – in Peters’ words, “the right to kill”.[38] Cast as an expansion of liberty, it simultaneously enlarges a sovereign power over disabled life. In this respect, Track 2 MaiD does not simply accommodate individual choice; it formalizes a hierarchy in which some lives are rendered negotiable within public policy.
Having assumed this formidable authority over disabled life, CAMAP has positioned itself as the architect and executor of the regime’s training apparatus, and in so doing has shown itself unwilling to engage with the implications of the power it now wields. When confronted with evidence that Track 2 MaiD is being used in cases where suffering stems from structural deprivation, internalized stigma, or unaddressed trauma, the institutional response has been to circle the wagons, narrow the frame, sanitize the language, and discredit the critics. CAMAP’s curriculum is a calculated response to political pressure, designed to pre-empt public concern by appearing rigorous while avoiding core ethical questions. The consequences are not abstract. Disabled people in Canada have died by Track 2 MaiD in circumstances that would have been preventable had their suffering been recognized for what it was: a response to marginalization, exclusion, and despair — not to their impairments. In rejecting the possibility of anti-ableist reform, CAMAP has entrenched a model in which clinicians are licensed to mistake social cruelty for incurable pain, and to treat death as the solution.
This chapter has attempted to document how that model was built, how critique was absorbed and deflected, and how a critical disability perspective was invited, then contained, and ultimately cast out by fiat[39]. My eventual resignation from Working Group 4[40] marked not only the end of critical engagement from within, but a structural limit on how far dissent could travel within a regime designed to insulate itself from disruption. What emerged from the experience was not a curriculum informed by equity, but a regime defined by its refusal of it. The final section now turns to a conclusion that places this regime in historical and ethical context, warning that the Canadian model of Track 2 MaiD may serve not as a beacon of “patient autonomy”, but as a case study in how ableism, once institutionalized, becomes impervious to reform.
Conclusion: The Curriculum That Would Not Learn
The expansion of MAiD in Canada to include persons who are not dying was justified, in part, by an appeal to medical professionalism. Its defenders argued that clinicians — governed by ethical codes, trained in careful assessment, and attuned to the complexities of suffering — could be trusted with the awesome power to authorize death. Yet what the CAMAP curriculum development process reveals is not a profession rising to this responsibility, but a regime working systematically to deflect and defeat it.
At each stage of curriculum design, where there might have been an opportunity for reflection or ethical pause, there was instead resistance. Resistance to naming the eugenic past of medicine. Resistance to acknowledging that suffering may be caused by structural ableism more than impairment. Resistance to considering the implications for MAiD assessment when the suffering of disabled patients is produced by social deprivation and sustained through political neglect. Most damningly, there was institutional denial of the possibility that the medical regime itself might be complicit in shaping, perpetuating, or misreading that suffering.
What has emerged under CAMAP’s stewardship is a model of medical authority in which the burden of responding to complex suffering — with care, imagination, and advocacy — is displaced. Rather than engaging with the social and existential dimensions of a patient’s suffering, the practitioner is trained to authorize its resolution through the mechanisms of consent and eligibility, culminating in the provision of MAiD. The moral and relational labour of tending to suffering is diverted, and the patient is left to carry the weight of what the system will not address. Capacity is defined in exclusively cognitive terms[41], voluntariness is assumed in the absence of overt coercion, and suffering — however forged by the slow violence of subjugation and abandonment — is treated as an interior, private phenomenon. In this model, the role of the assessor is not to interrogate how power shapes desire, but to verify that the desire for death is sufficiently polished to pass as rational.
But Track 2 MAiD is not merely a clinical matter. It is a political regime in which disabled people — especially those without economic or social advantage — have become uniquely exposed to the normalization of death as a ‘therapeutic’ response to marginalization. In the absence of comprehensive supports, secure housing, adequate income, or the affirmation of a non-degraded place in the world, death appears not as an autonomous choice, but as an induced inevitability.[42] That CAMAP’s training materials refuse to consider this context is not a pedagogical lapse. It is a profound institutional failure of moral perception.
This failure is not only theoretical; it reverberates in the lives of disabled people now living under the shadow of Track 2. When a disabled adolescent in state care is deemed eligible for MAiD rather than offered protection from abuse; when a young man despairs of dating and dies with the blessing of medical authority; when a woman with a spinal cord injury comes to see toileting assistance as a degradation and finds this view unchallenged by those empowered to intervene — these are not triumphs of autonomy. They are the outcomes of a regime that has disavowed its obligation to imagine alternatives.
And they are outcomes that are, increasingly, beyond contest. CAMAP has consolidated its authority as both educator and gatekeeper. Its curriculum, funded by the federal government[43] and endorsed by national regulatory bodies, is the tool through which clinical norms are established, legitimized, and reproduced. It is not simply that ableist assumptions survive within this curriculum; it is that the curriculum was deliberately structured to ensure they would not be meaningfully challenged. Where critique might have created openings for ethical discernment or institutional humility, it was muted, reframed, or erased.
The result is not impartial. It is an ableist regime with the imprimatur of neutrality — one that trains clinicians to treat as natural what is in fact the product of social abandonment and systemic failure. The insistence on sanitized, apolitical language is not an act of restraint, but of obfuscation. In this regime, it is considered inappropriate to speak of eugenics, dangerous to link disability to eligibility, and unprofessional to suggest that some suffering is a response to injustice, not biology. The message is clear: death is a solution medicine can offer, but context is not a reality it must face.
As Hilary Pearson has observed in her close reading of Health Canada’s Fifth Annual Report on Medical Assistance in Dying[44], the federal government frames its mandate as achieving population health “as measured by longevity, lifestyle and effective use of the public health care system,” even as it reports, in sanitized statistical terms, the thousands of deaths accomplished through MAiD.[45] Pearson reads this juxtaposition as symptomatic of a “healthist” logic in which death can be narrated as an outcome of system efficiency rather than as an index of social abandonment. That tension — between commitments to longevity and the normalization of assisted death for disabled persons — haunts Canada’s expanded MAiD regime.
My resignation from the CAMAP working group[46] was not the loss of a seat at the table — it was the collapse of any illusion that the table was meaningfully shared. The curriculum’s final form is the product of institutional consolidation. Attempts to introduce anti-ableist analysis were treated not as contributions to ethical discourse, but as threats to institutional coherence. Anti-ableist insights were reframed as “lived experience,” their arguments as “personal values,” and their structural critiques as political agendas incompatible with the ostensibly neutral goals of education.
But education is never neutral. And neutrality, in this context, is not a position of fairness but a mechanism of evasion. By constructing its training around the refusal of context, CAMAP has ensured that Track 2 MAiD will remain impervious to reform. For experienced practitioners, serious engagement with anti-ableist critique would require revisiting past assessments — and confronting the possibility that decisions made in good faith have resulted in avoidable deaths. This is no small reckoning. As one working group member observed, such reflection is not only professionally destabilizing but morally unbearable. The regime’s defensiveness is, in part, a strategy of survival — preserving not just a practice, but the psychic stability of those who have participated in it. Thus the curriculum does not merely avoid structural critique; it preempts the very conditions necessary for such critique. The law, by contrast, remains subject to challenge[47] — and may now be the only domain in which equitable reform is still conceivable. What Canada’s MAiD regime cannot do — what it has shown again and again that it cannot withstand — is to be in conversation with disability justice, or even to reckon with the presence of those who refuse to stop speaking its language.
If Track 2 MAiD in Canada is now regarded internationally as a cautionary tale[48], it is not only because the law permits non-dying disabled people to seek assisted death, but because the institutional culture surrounding that law has rendered critique so easily dismissible. The medical regime does not merely tolerate Track 2 — it defends it, instructs others in how to practice it, and resists all efforts to expose its premises to ethical scrutiny. It does so under the authority delegated to it by the state – an authority that has been exercised not with careful stewardship, but with professional abdication.
There remains, however, a record. A record of resistance, of questions raised, of silences documented.[49] This chapter contributes to that record. It does not offer a blueprint for reform, because reform, under current conditions, is foreclosed. It offers instead a clear view of how ableism has been institutionalized — through a calculated refusal to confront the social, ethical, and epistemological conditions of disabled people’s suffering. It is a record written in grief, frustration, and the clarity born of seeing power unmasked – the clarity of knowing that in Canada today, under the auspices of medical expertise, some lives are made more killable because of how disability is understood.
The cultural norms and structural authorities that enabled this regime long predate the law, and they will long outlast it. But what is made visible through this story is the cost of abandoning the critical capacities that ought to animate any practice involving life and death. The CAMAP curriculum does not merely neglect those capacities. It trains practitioners to turn away from them.
That turning away, and its consequences, will continue to reverberate until the system itself is finally called to account.
Endnotes
- AAn Act to amend the Criminal Code (medical assistance in dying), S.C. 2021, c. 2, amending Criminal Code, R.S.C. 1985, c. C-46, s. 241.2.
- For a detailed account of this opposition, see Frazee, C. (2024). MAID Resistance in Canada: Sounding the Five-Minute Entreaty. Canadian Journal of Disability Studies, 13(2), 1–175.
- Valentina Capurri, “Eugenics under Another Name,” Canadian Journal of Disability Studies 14(1) (2025) 45-70; Heidi Janz, “MAID to Die by Medical and Systemic Ableism,” In: Kotalik, J., Shannon, D.W. (eds) Medical Assistance in Dying (MAID) in Canada. The International Library of Bioethics, vol 104. Springer, Cham, Switzerland; Hansen, N. (2022). DisAppearing disability: Disability MAiD invisible. In T. Titchkosky, E. Cagulada, M. DeWelles, & E. Gold (Eds.), DisAppearing: Encounters in Disability Studies (pp. 212-223). Canadian Scholars; Michele Hutyra, “An Inaccessible Life but Endorsed Death: Examining the biopolitics of Canada’s medical assistance in dying (MAID)” Young Anthropology – Undergraduate Student Journal of Anthropology Vol. 5, pp. 1-10 (Fall 2024). Department of Anthropology, University of Toronto; Hilary Pearson, “Disability, Sovereignty, and the Politics of Death: Interpreting MAID (Medical Assistance in Dying) Through a Critical Disability Studies Lens. Canadian Journal of Disability Studies, 14(2), 96–129 (2025); Gabrielle Peters, “Creating a Killable Class and Manufacturing Selective Suicidality: Thoughts of a Past and Future Ironing Board”, in Coelho, Ramona, et al. Unravelling MAiD in Canada: Euthanasia and Assisted Suicide As Medical Care, McGill-Queen’s University Press, 2025.
- Alexandre Baril, “Suicidism: A new theoretical framework to conceptualize suicide from an anti-oppressive perspective,” Disability Studies Quarterly 2020, 40(3).
- Fiona Kumari Campbell, Contours of Ableism: The Production of Disability and Abledness (London: Palgrave Macmillan, 2009).
- Talila Lewis, “Working Definition of Ableism,” updated 2022, https://www.talilalewis.com
- Shelley Tremain, Foucault and the Government of Disability, 2nd ed. (Ann Arbor: University of Michigan Press, 2015).
- Jasbir K. Puar, The Right to Maim: Debility, Capacity, Disability (Durham, NC: Duke University Press, 2017); Nirmala Erevelles, Disability and Difference in Global Contexts: Enabling a Transformative Body Politic (New York: Palgrave Macmillan, 2011).
- Alison Kafer, Feminist, Queer, Crip (Bloomington: Indiana University Press, 2013).
- Carter v. Canada (Attorney General), 2012 BCSC 886 at para 1239.
- Ibid at para 1240; aff’d Carter v. Canada (Attorney General), 2015 SCC 5.
- Heidi L. Janz, “Ableism: the undiagnosed malady afflicting medicine,” CMAJ 191, no. 17 (2019): E478–E479.
- Canadian Association of MAiD Assessors and Providers (CAMAP), Foundations of MAiD in Canada, Topic 1: “Various Perspectives on the Legalization of MAiD.” Online curriculum module accessed May 3, 2024. Private access via CAMAP Brightspace platform. Screenshot taken by the author.
- Critical disability studies, for example, does not present a binary “for” or “against” MAiD position, but a sustained structural analysis of how ableism, sanism, neoliberalism, and class power shape whose lives are deemed worth living. Alexandre Baril has argued that contemporary assisted dying regimes simultaneously normalize death for those cast as unproductive or “unsalvageable,” while pathologizing and disciplining suicidal persons deemed capable of reintegration into the neoliberal order. Even from positions that diverge sharply on the policy question of assisted dying, disability scholars converge in identifying the differential valuation of lives under conditions of structural inequality. Alexandre Baril, “The Somatechnologies of Canada’s Medical Assistance in Dying Law: LGBTQ Discourses on Suicide and the Injunction to Live,” Somatechnics 7, no. 2 (2017): 203-205.
- My entry into Working Group 4 was through an invitation extended in June 2021 by Dr. Madeline Li, the working group’s chair. Dr. Li’s approach was collegial and principled, reflecting a commitment to inclusive dialogue rather than institutional positioning. What unfolded during the curriculum development process, however, revealed limits to collaboration that reflected structural dynamics beyond her individual intent.
- Gabrielle Peters, “Creating a Killable Class and Manufacturing Selective Suicidality”, pp. 206, 210-213. Peters dismantles the myth of the socially unencumbered chooser as a paradigm of 'astroturf autonomy' – autonomy that appears lush and natural but is artificial, constructed, and policy-conditioned.
- "Robin Interview Transcript and Screenplay,” working draft shared with the author by CAMAP Working Group 4, April 16, 2023. The quoted passage was essentially preserved without substantive change in the final recorded video. However, sometime after my resignation from the working group, the module was restructured and I have been told that this video was not used.
- When I raised questions about whether Robin's despair might be mitigated through environmental adaptations, peer mentorship, employment reintegration, or disability-affirming therapeutic support, I was told that such avenues would be pursued in practice and therefore did not need to be reflected in this educational scenario.
- For an analysis of ableism as embedded within our social architecture and as evident in Canada's expanded MAiD law, see Isabel Grant, “Legislated Ableism: Bill C-7 and the Rapid Expansion of Medical Assistance in Dying in Canada,” McGill Journal of Law & Health 15, no. 2 (2024): 293–302.
- Heidi Janz, " Ableism: the undiagnosed malady afflicting medicine,” 2019.
- Canadian MAiD Curriculum Glossary, accessed May 13, 2025, via CAMAP Brightspace platform for registered practitioners. Last modified September 22, 2023.
- The changes described in this section were made after my resignation from the working group in August 2023.
- Catherine Frazee, original draft definitions of “Ableism” and “Anti-Ableism,” submitted to CAMAP Working Group 4, April 24, 2023. Both definitions were subsequently abridged in the final version of the Canadian MAiD Curriculum glossary.
- Ibid.
- Slide authored by Catherine Frazee, February 4, 2023, for consideration by the CAMAP Module 4 Working Group. One of three discussion questions proposed to support critical reflection on ableism in the context of MAiD assessment. This slide was not retained in the final curriculum.
- Fiona Kumari Campbell, Contours of Ableism; Talila Lewis, Working Definition of Ableism; Heidi Janz, MAID to Die by Medical and Systemic Ableism. Campbell conceptualizes ableism as a structuring logic that casts disability as diminished humanity; Lewis expands this to show how value is assigned to bodies and minds within racialized and capitalist hierarchies; and Janz traces how such assumptions pass as neutral clinical judgment. In this framework, suffering attributed to disability cannot be analytically separated from the social and material arrangements that produce precarity.
- Case reports that illustrate the influence of poverty, isolation, and systemic vulnerability on MAiD requests include: Darren Bernhardt, “Winnipeg Woman with ALS Chooses Medically Assisted Death after Futile Bid for Home Care,” CBC News, October 11, 2022, https://www.cbc.ca/news/canada/manitoba/sathya-dharma-kovac-als-medical-assistance-in-death-1.6605754; Bethany Lindsay, “He Chose a Medically Assisted Death after Struggling to Find Adequate Care,” CBC News, August 2, 2019, https://www.cbc.ca/news/canada/british-columbia/als-bc-man-medically-assisted-death-1.5244731. Additional cases are documented by the group Living with Dignity at https://living-with-dignity.ca/remembering-lives-lived/. Further examples and discussion of structural inequalities, poverty and lack of supports shaping MAiD requests can be found in Grant, "Legislated Ableism", pp. 259–334. Pearson also recounts cases where MAiD was pursued to relieve the suffering of sustained material precarity. Pearson, "Disability, Sovereignty and the Politics of Death" (2025) pp. 120-121.
- See Grant's critique of the legal fiction of autonomous choice in conditions of profound structural inequality in Grant, “Legislated Ableism,” 324-331.
- Canada’s MAiD legislation includes a preamble that affirms the importance of “ensuring that appropriate safeguards are in place, having regard to the vulnerability of persons who may seek medical assistance in dying,” and recognizes “the need to protect those who may be vulnerable to being induced to end their lives in a moment of weakness.” Criminal Code, RSC 1985, c C-46, s 241.1 et seq., as amended by An Act to amend the Criminal Code (medical assistance in dying), SC 2016, c 3 and SC 2021, c 2.
- Ibid.
- The statutory criteria for MAiD eligibility require that a person have a “grievous and irremediable medical condition” that “causes enduring physical or psychological suffering that is intolerable to them and […] cannot be relieved under conditions that they consider acceptable.” Criminal Code, RSC 1985, c C-46, s 241.2(2)(c). However, the legislation does not define the concept of “causes,” nor does it provide specific criteria for distinguishing between suffering that is directly attributable to a person’s medical condition and suffering that is compounded or produced by social, economic, or structural factors. There is similarly no mandated guidance on how assessors are to weigh multiple potential causal contributors or adjudicate their relative significance, leaving clinicians with significant interpretive discretion in assessing causation under the statute.
- As Grant notes, suffering cannot be reduced to the symptoms accompanying a disability; access to the social determinants of health profoundly shapes whether a life with impairment is experienced as tolerable or intolerable. When such determinants are ignored, the distinction between medical causation and social production of despair collapses. Grant, I. (2025). Why Track 2 MAiD is Discriminatory. Canadian Journal of Bioethics / Revue canadienne de bioéthique, 8(4), 45–55, p. 46.
- Recent case analyses published in BMJ Supportive & Palliative Care further document systemic weaknesses in the application of Canada’s MAiD safeguards. Drawing on anonymized cases reviewed by the Ontario Chief Coroner’s MAiD Death Review Committee, Coelho, Shannon, and Lemmens describe lax interpretations of “reasonably foreseeable death,” inadequate exploration of reversible suffering, unreliable capacity assessments, and cases in which caregiver burnout or psychosocial distress appeared to influence eligibility determinations. Coelho, R., Shannon, D., & Lemmens, T. (2026). Safeguard failures in Canada’s MAiD system. BMJ Supportive & Palliative Care, 0, 1–3.
- Grant, "Why Track 2 MAiD Is Discriminatory" (2025), p. 45.
- Peters situates this precarity as the predictable outcome of policy decisions that have rendered disabled people “unintended participants” in a society designed without them.³ In such a context, suffering cannot be cleanly attributed to impairment alone. It is produced at the intersection of disability, economic abandonment, and institutional design. To treat that suffering as solely medical is to misrecognize its source. Peters, "Creating a Killable Class," pp. 227-233.
- As Grant observes, Track 2 widens the gap between how we respond to the suffering of disabled persons and how we respond to others: once suffering is even partly grounded in an irremediable condition, death may be treated as an appropriate response “regardless of the role of social factors in that suffering." Grant, "Why Track 2 MAiD Is Discriminatory" (2025) p. 47.
- Yet, as Grant has argued, deciding whose suffering warrants a response of death “is fundamentally not a medical decision but a normative one about whose lives may be worse than death.” The framing of this determination as clinical expertise masks the evaluative judgment at its core. See Grant, "Why Track 2 MAiD Is Discriminatory" (2025), p. 46.
- Peters, "Creating a Killable Class," p. 206.
- See Catherine Frazee, memorandum to Dr. Madeline Li, August 18, 2023. The letter details a series of unilateral directives issued by the CMCDC, including orders to de-centre the concept of vulnerability, to remove controversial content rather than engage with it, and to eliminate all references to eugenics. These measures, taken together, marked a categorical rejection of anti-ableist critique and a shift toward a curriculum stripped of nuance, ethical inquiry, and structural analysis. The letter includes the author’s resignation from Working Group 4, submitted in response to these actions. On file with the author.
- I would not be the only member to resign from Working Group 4. I have since learned that Dr. Li (the Working Group Chair), and the Medical Ethicist in our group resigned separately some time after my departure. Personal communication with Dr. Madeline Li, November 16, 2025.
- Even so, as Coelho and colleagues note, some documented cases have involved individuals with delirium or advanced dementia receiving MAiD following capacity assessments that would not meet the rigor expected in other high-stakes legal contexts. Coelho et al., "Track 2 MAiD and Assessors' Decision-Making" (2026), pp. 1-3.
- Where choices are driven by state-sanctioned poverty, social isolation, trauma, loneliness, or perceived burdensomeness, construing assisted death as an expression of autonomy obscures the conditions that produced it. As Grant cautions, a choice may be the only available option and yet not meaningfully autonomous. Grant, "Why Track 2 MAiD Is Discriminatory" (2025), p. 48.
- In 2022, Canada’s Minister of Health, Jean-Yves Duclos, disclosed that $3.3 million in federal funding had been provided to the Canadian Association of MAiD Assessors and Providers (CAMAP) for the development of a national MAiD curriculum to deliver “high quality MAiD training to healthcare practitioners across Canada.” See Department of Health, Government Response to the First Report of the Special Joint Committee on Medical Assistance in Dying, October 2022, https://www.parl.ca/content/Committee/441/AMAD/GovResponse/RP11995101/441_AMAD_Rpt01_GR/DepartmentOfHealth-e.pdf.
- In its Fifth Annual Report on Medical Assistance in Dying in Canada, Health Canada presents detailed statistics on MAiD requests, assessments, and provisions for the 2023 calendar year — including new information collected under the updated monitoring regulations that came into force on January 1, 2023. The data is presented through a reassuringly technocratic framing that for the most part obscures the social conditions under which these deaths have occurred and presents MAiD mortality as a favourable measure of regime performance. See Health Canada, Fifth Annual Report on Medical Assistance in Dying in Canada (2023) (Government of Canada, 2024), online: https://www.canada.ca/en/health-canada/services/publications/health-system-services/annual-report-medical-assistance-dying-2023.html
- Pearson, "Disability, Sovereignty, and the Politics of Death" (2025), pp. 100-103 and 116-117.
- See Frazee, memorandum to Dr. Madeline Li, August 18, 2023, cited above at note 10. The letter includes the author’s formal resignation from Working Group 4 and describes the final module as “gutted,” denouncing the process as ideologically driven and structurally dismissive of disability rights perspectives. On file with the author.
- See K.C. et al. v. His Majesty the King in Right of Canada, Notice of Application filed September 25, 2024, Ontario Superior Court of Justice, Court File No. CV-24-0072847-0000. The applicants — two individuals and four national disability rights organizations — challenge the constitutionality of Canada’s Track 2 MAiD regime under sections 7 and 15 of the Canadian Charter of Rights and Freedoms, arguing that it discriminates against disabled persons and violates their right to life and security of the person. Available at JURIST, https://www.jurist.org/news/wp-content/uploads/sites/4/2024/09/issued_fresh_as_amended_notice_of_application_k.c._v._canada_.pdf.
- This concern is increasingly voiced by international human rights bodies, disability advocates, and ethical observers of end-of-life practice. See Committee on the Rights of Persons with Disabilities, Concluding Observations on the initial report of Canada, CRPD/C/CAN/CO/1, 9 May 2022, paras. 42–43, https://digitallibrary.un.org/record/3979989. See also Michael Coren, “I thought assisted dying was merciful, now it’s terrifying,” The Times, November 12, 2024, https://www.thetimes.co.uk/article/assisted-dying-merciful-canada-terrifying-6jg55drsg.
- This article and the scholarship it cites are not isolated laments but part of a documented archive of resistance and critique from disabled and disability-aligned voices. Contributions to this record range from parliamentary testimony and personal narrative to critical scholarship — all insisting that disabled experience and structural critique be taken seriously in the MAiD debate. Among these, the Canadian Journal of Disability Studies dedicated an entire volume to Medical Assistance In Dying: Resistance in Canada (Vol. 13 No. 2, 2024), assembling testimonial statements and critical interventions entered into the parliamentary record and the broader public debate prior to the 2021 expansion of MAiD law — a collective insistence that disabled perspectives be foregrounded rather than eclipsed. Available: https://cjds.uwaterloo.ca/index.php/cjds/issue/view/47
References
- Baril, Alexandre. Suicidism: a new theoretical framework to conceptualize suicide from an anti-oppressive perspective. Disability Studies Quarterly. 2020;40(3).
- Baril, Alexandre. The Somatechnologies of Canada's Medical Assistance in Dying Law: LGBTQ Discourses on Suicide and the Injunction to Live Somatechnics 2017 7:2, 201-217
- Capurri, Valentina. (2025). Canada’s Medical Assistance in Dying: Eugenics Under Another Name? Canadian Journal of Disability Studies, 14(1), 45–70.
- Campbell, Fiona Kumari. Contours of Ableism : The Production of Disability and Abledness. Palgrave Macmillan, 2009.
- Campbell, Fiona Kumari. Exhausted Lives - Expulsions via On Demand Euthanasia: Implications of Self Determination Theory- The Joint Social Work Education and Research Conference , 15 June 2023, Glasgow, Keynote Address. [Online]. https://www.academia.edu/103628807/Exhausted_Lives_Expulsions_via_On_Demand_Euthanasia_Implications_of_Self_Determination_Theory
- Coelho, Ramona; Lemmens, Trudo; Shannon, David. “Track 2 MAiD and Assessors’ Decision-Making, We Need More Than Internal MAiD Clinician Consensus” CMAJ 198 (1) January 14, 2026.
- Coelho, Ramona; Shannon, David; Lemmens, Trudo. “Safeguard Failures in Canada’s MAiD System” BMJ Supportive & Palliative Care 2026;0:1–3.
- Erevelles, Nirmala. Disability and Difference in Global Contexts : Enabling a Transformative Body Politic. Palgrave Macmillan, 2011.
- Frazee, Catherine. (2024). MAID Resistance in Canada: Sounding the Five-Minute Entreaty. Canadian Journal of Disability Studies, 13(2), 1–175.
- Grant, Isabel. “Legislated Ableism: Bill C-7 and the Rapid Expansion of Medical Assistance in Dying in Canada” (2024) 15:2 McGill JL & Health 259.
- Grant, Isabel. (2025). Why Track 2 MAiD is Discriminatory. Canadian Journal of Bioethics / Revue canadienne de bioéthique, 8(4), 45–55.
- Grant, Isabel, Janine Benedet, Elizabeth Sheehy, and Catherine Frazee. "A Conversation on Feminism, Ableism, and Medical Assistance in Dying." Canadian Journal of Women and the Law 35, no. 1 (2024): 31-72.
- Hansen, Nancy. (2022). DisAppearing disability: Disability MAiD invisible. In T. Titchkosky, E. Cagulada, M. DeWelles, & E. Gold (Eds.), DisAppearing: Encounters in Disability Studies (pp. 212-223). Canadian Scholars.
- Hutyra, Michele. “An inaccessible life but endorsed death: Examining the biopolitics of Canada’s medical assistance in dying (MAID)” Young Anthropology – Undergraduate Student Journal of Anthropology Vol. 5, pp. 1-10 (Fall 2024). Department of Anthropology, University of Toronto Mississauga
- Janz, Heidi. (2023). MAID to Die by Medical and Systemic Ableism. In: Kotalik, J., Shannon, D.W. (eds) Medical Assistance in Dying (MAID) in Canada. The International Library of Bioethics, vol 104. Springer, Cham, Switzerland.
- Janz, Heidi. (2023). Plagued to Death by Ableism: What the COVID-19 Pandemic and the Expansion of Eligibility for MAID Reveal About the Lethal Dangers of Medical and Systemic Ableism in Canada. Canadian Journal of Bioethics / Revue canadienne de bioéthique, 6(3-4), 137–141.
- Janz, Heidi. “Ableism: The Undiagnosed Malady Afflicting Medicine” (2019) 191:17 Can Medical Assoc J E478 at E479.
- Lewis, Talila. Working Definition of Ableism – January 2022 Update [Online]. https://www.talilalewis.com/blog/working-definition-of-ableism-january-2022-update
- Medical Assistance In Dying: Resistance in Canada. 2024. Canadian Journal of Disability Studies 13, no. 2. [Online]. https://cjds.uwaterloo.ca/index.php/cjds/issue/view/47
- Pearson, Hilary. (2025). Disability, Sovereignty, and the Politics of Death: Interpreting MAID (Medical Assistance in Dying) Through a Critical Disability Studies Lens. Canadian Journal of Disability Studies, 14(2), 96–129.
- Peters, Gabrielle. (2024) “Reality, not religion, is the reason people need MAiD-free health care” Policy Options April 26, 2024. [Online]. https://policyoptions.irpp.org/2024/04/maid-free-health-care/
- Peters, Gabrielle. “creating A Killable Class and Manufacturing Selective Suicidality: Thoughts of a Past and Future Ironing Board”, in Coelho, Ramona, et al. Unravelling MAiD in Canada: Euthanasia and Assisted Suicide As Medical Care. Edited by Trudo Lemmens et al., 1st ed., McGill-Queen’s University Press, 2025.
- Puar, Jasbir. The Right to Maim: Debility, Capacity, Disability. Duke University Press, 2017.
- Tremain, Shelley. (2020) Submission to the Standing Senate Committee on Legal and Constitutional Affairs, November 23, 2020. [Online]. https://sencanada.ca/content/sen/committee/432/LCJC/Briefs/ShelleyTremain_e.pdf
- Tremain, Shelley. Ed., Foucault and the Government of Disability (Ann Arbor: University of Michigan Press, 2005).
- Tremain, Shelley. “Disaster Ableism, Epistemologies of Crisis and the Mystique of Bioethics”, in Shelley Lynn Tremain. The Bloomsbury Guide to Philosophy of Disability. Bloomsbury Academic, 2024.