Assessing Teachers’ Knowledge and Competence in Supporting Neurodivergent Students in Ghana’s Inclusive Education Schools
Évaluer les connaissances et les compétences du personnel enseignant dans le soutien aux élèves neurodivergents dans les écoles d’éducation inclusive au Ghana
Valda Deide Commey, MPhil
Department of Psychology, University of Ghana
0000-0002-7961-4157
Mabel Oti-Boadi, PhD
Department of Psychology, University of Ghana
0000-0001-5892-9021
moti-boadi [at] ug [dot] edu [dot] gh
Benjamin Amponsah, PhD
Department of Psychology, University of Ghana
0000-0002-2597-4229
Kenneth Owusu Ansah, MPhil
Seven Hills Foundation, Worcester- Massachusetts USA
0000-0002-5311-3004
Abstract
This study assessed the knowledge and competence of teachers in inclusive education schools in Ghana in supporting children with neurodivergent (ND) conditions, including autism spectrum disorder (ASD), learning disability, and cerebral palsy. A quantitative cross-sectional survey was conducted with 150 teachers from 46 basic schools, sampling from both public and private institutions through Special Education Needs coordinators. Teachers completed measures assessing their knowledge of each ND condition, as well as the Learning in Regular Classroom Teacher's Professional Competency Scale. Results from multivariate analysis showed significant differences in competence dimensions among teachers of children with different neurodivergent conditions. Teachers of children with cerebral palsy exhibited the highest levels of competence across attitudes, knowledge, skills, and autonomy. While teachers demonstrated above-average ASD and cerebral palsy knowledge, learning disability knowledge was below average. Teacher knowledge of ASD showed significant positive correlations with skills, pedagogical knowledge, and agency. Knowledge of learning disabilities correlated positively with skills, pedagogical knowledge, and agency. The findings highlight areas requiring comprehensive in-service teacher training on neurodivergent conditions and inclusive instructional strategies to enhance teacher preparedness in Ghana's inclusive education policy framework.
Keywords: Knowledge, Neurodivergence, Inclusive Education
Résumé
Cette étude a évalué les connaissances et compétences des enseignantes et enseignants d’écoles d’éducation inclusive au Ghana dans le soutien aux enfants présentant des conditions neurodivergentes, dont le trouble du spectre de l’autisme (TSA) et les troubles d’apprentissage, ainsi que la paralysie cérébrale. Une enquête quantitative transversale a été menée auprès de 150 enseignantes et enseignants issus de 46 écoles de base, recrutés dans des établissements publics et privés par l’intermédiaire du personnel coordonnant les besoins en éducation spécialisée. Elles et ils ont rempli des mesures évaluant leurs connaissances de chaque condition ainsi que l’échelle Learning in Regular Classroom Teacher’s Professional Competency Scale. Les analyses multivariées ont révélé des différences significatives entre les dimensions de compétence, selon la condition des enfants. Les enseignantes et enseignants d’enfants ayant une paralysie cérébrale présentaient les niveaux les plus élevés en attitudes, connaissances, habiletés et autonomie professionnelle. Les connaissances liées au TSA et à la paralysie cérébrale étaient supérieures à la moyenne, tandis que celles portant sur les troubles d’apprentissage étaient inférieures. Les connaissances sur le TSA étaient positivement corrélées aux habiletés, aux connaissances pédagogiques et à l’agentivité, tout comme celles sur les troubles d’apprentissage. Les résultats soulignent la nécessité d’une formation continue approfondie pour les enseignantes et enseignants sur les conditions neurodivergentes et les stratégies pédagogiques inclusives afin de renforcer leur préparation dans le cadre de la politique ghanéenne d’éducation inclusive.
Mots-clés : Connaissances, neurodivergence, éducation inclusive
Introduction
Neurodivergence encompasses a spectrum of conditions that manifest early in a child's life, affecting various aspects of cognitive, behavioural, and motor functioning (APA, 2022; de Villiers, 2023). Common neurodivergent conditions include Autism Spectrum Disorder (ASD), characterized by differences in social communication and repetitive behaviours; learning disabilities, which affect the acquisition and use of skills related to listening, speaking, reading, writing, reasoning, or mathematical abilities (APA, 2022); and cerebral palsy, a group of permanent movement-related conditions appearing in early childhood (Carriba et al., 2023). Globally, the prevalence of neurodivergent conditions among school-aged children and adolescents is on the rise, with significant implications for educational practices and societal inclusion (Aldharman et al., 2023; Yoro et al., 2020). In Ghana, the traditional approach involved placing neurodivergent children in specialized schools, while mainstream schools primarily served neurotypical students (Azupogo et al., 2023; Duorinaah, 2023). This practice led to concerns about marginalization and exclusion, which spurred a shift towards inclusive education. Introducing the Inclusive Education Policy (IEP) marked a pivotal change in Ghana’s educational landscape, aiming to integrate children with diverse needs into inclusive education schools and foster a culture of diversity and inclusion (MOE, 2015; Vanderpuye et al., 2018). Since its inception, the IEP has witnessed significant expansion, with over 3,000 schools embracing inclusive practices nationwide (Deku & Vanderpuye, 2017).
The implementation of inclusive education policies continues to face challenges that contribute to the difficulties experienced by neurodivergent students. These challenges often stem from systemic and policy-related factors within the education system. Research highlights that teachers often lacked adequate knowledge and specialized skills to support students with conditions such as ADHD, ASD, dyspraxia, and dyslexia effectively (Gómez-Marí et al., 2021; Yoro et al., 2020). Additionally, negative attitudes and insufficient training among educators can impact on the academic success and overall well-being of these students (Arthur & Chen, 2023; Asamoah et al., 2023; Nti-Adarkwah et al., 2023). To address these issues, targeted professional development and in-service education are necessary to enhance teachers' competence and foster positive attitudes towards neurodivergent students (Dickson et al., 2020; Knochel et al., 2020; Sheriff et al., 2022).
Although some research has explored teachers’ knowledge and attitudes towards inclusive education and neurodivergent conditions in Ghana, there remains a gap in understanding how teachers manage a wider range of neurodivergent conditions within the inclusive education framework (Baidoo et al., 2023; Kotor et al., 2022; Sheriff et al., 2022). This study aims to address this gap by evaluating the knowledge and competence of teachers in inclusive education settings in supporting students with neurodivergent conditions, including ASD, learning disabilities, and cerebral palsy. The study will specifically examine differences in teacher competence and the relationship between knowledge of neurodivergent conditions and their ability to effectively support these students.
By shedding light on the subtleties of inclusive education and identifying areas for improvement, this study contributes to the ongoing efforts to create an equitable and inclusive educational environment for all children in Ghana. Through evidence-based interventions and policy reforms informed by empirical research, Ghana can continue its journey towards realizing the full potential of inclusive education and ensuring that every child, regardless of ability, has access to quality education and opportunities for meaningful participation in society.
Methods
Research Design
The current study used a croѕѕ-ѕectional design to study teachers teaching children with ND conditions in mainstream institutions. The cross-sectional design is well-suited for capturing a moment-in-time view of teachers’ experiences and attitudes towards teaching children with ND conditions in mainstream classrooms. Collecting data at a single point can efficiently describe the current state of teachers’ preparedness, challenges, and attitudes. This provides a rich, immediate understanding of these variables, particularly useful in contexts where attitudes and practices may evolve over time due to policy changes or training initiatives.
Participants
Using purposive sampling techniques, this project selected 150 public and private teachers from 46 Ghanaian schools in the Greater Accra and Eastern Regions of Ghana. Teachers in mainstream private and government schools who have currently implemented inclusive education in their schools based on the Ministry of Education ([MOE], 2015) recommendations and had at least one student diagnosed with ASD, learning disability, or cerebral palsy in their classroom at the time of the study were recruited. Participants were recruited from 29 public schools and 17 private schools in selected districts of Greater Accra and Eastern Regions in Ghana. The final sample completed either an online survey (created with Google Forms) or a paper-and-pencil survey. A response rate of 92% constituting 150 questionnaires was retrieved, but only 113 of the returned questionnaires met the inclusion criteria. The age of the participants ranged from 24 to 57 years. There were 50 male teachers (44.25%) and 63 female teachers (55.75%), with 50 (44.2%) managing children with ASD, 43 (38.1%) managing children with LD, and 20 (17.7%) managing children with cerebral palsy. Sixty-seven of these teachers (59.3%) worked in public schools, with the remaining 40.7% working in private schools. Participants’ teaching experience ranged from 1 to 30 years. Fifty-five teachers (48.7%) had diploma certificates.
Measures
A demographic questionnaire was included in the instruments of the study to obtain relevant demographic data about the teachers. Their details included gender, type of mainstream sector, qualification, and type of ND children they teach.
The LRC Teachers’ Professional Competency Scale (Mu et al., 2015): This scale comprises 28 items and evaluates teachers’ knowledge, skills, attitudes, and agency towards managing neurodivergent children in mainstream settings. The scale was adapted by changing the word disability to NDD (for neurodivergent disorder) and piloted before being used in the main study. Participants were asked to respond by indicating their competency across a 5-point Likert-type scale (1 = “strongly agree” and 5 = “strongly disagree”). Mu et al.’s (2015) study demonstrated a sound alpha coefficient of .94 and obtained .89, .89, .90, and .83 for each subsection. The scale revealed an overall alpha of .85 in the current study.
Responses on the LRC Teachers’ Professional Competence scale were scored by firstly reverse scoring all items on the scale to obtain a positive direction of scores and then generating a total score of the 28 items. The minimum score on the scale was 68 and the maximum score was 140. A score of 28 to 56 on the LRC Teachers’ Professional Competence scale thus, depicted adaptive competence (i.e. minimal score), 57 to 111 represented reproductive competence (i.e. moderate score), and 112 to 140 for optimal competence (i.e. higher score) (Zulfija et al., 2013).
The Autism Knowledge Questionnaire (Haimour & Obaidat, 2013): This also consists of 30 items that test teachers' understanding of the causes, manifestations, and management of autism. Participants express their knowledge by selecting True, False, or Don't Know. The test reported an alpha of .92 (Haimour & Obaidat, 2013). The scale had an alpha value of .83 in the current study.
The Learning Disability Questionnaire (Kidd, 2000): This scale consists of 30 items that assess teachers' perceptions of learning disabilities, its forms, causes, characteristics, and management. The test has three response sets of True/False/Don’t Know. Kidd (2000) found an acceptable alpha coefficient of.80. and .74 in the current study.
The Knowledge of Cerebral Palsy Questionnaire (Dambi et al., 2017): This scale consists of 20 knowledge statements with three choices for respondents to pick from True, False, and Don't Know. The questionnaire evaluates many aspects of cerebral palsy knowledge, such as definition, aetiology, presentation, and management. The study by Dambi et al. (2017) indicated a sound alpha coefficient of .80. The current study also yielded a sound alpha of .86
Scoring
All questions presented on the knowledge scales were given as True/False statements and a Don’t Know option which respondents were urged to pick rather than guessing the correct response. In scoring the knowledge scales, correct responses were separated from incorrect ones using information given by the test developers which were also verified using DSM-5 and other reliable academic sources. A correct response was given a score of 2 and an incorrect response was scored 0. The highest score thus was 60 on the autism knowledge and learning disability knowledge scales and 40 on the cerebral palsy knowledge scale and the least score was 0. Higher levels and lower levels of knowledge were determined using the median split technique suggesting that scores below the median scores on these scales represent low levels of knowledge and scores above the median scores represent higher levels of knowledge.
Procedure
Teachers consented to participate in the study after the details of the study (including potential risks and benefits, privacy, and confidentiality) were thoroughly explained to them. The lead investigator administered the questionnaires at various inclusive education schools. The data were collected using both online and paper-and-pencil format. For the online surveys, Google Forms were used to obtain responses from teachers who were far to reach or were on vacation. In doing so, a link was shared to either their emails or social media platforms (particularly WhatsApp). Paper-and-pencil questionnaires were to obtain responses from teachers who were in school and were easily accessible to the researcher. Participation was entirely voluntary, and teachers were not compensated for their participation. Data collection spanned a period of three months (July-September 2021).
Data Analysis
We first assessed the normality of score distributions using basic statistical methods. The skewness, kurtosis, and outliers of the continuous variables were examined for normality. Skewness shows whether the scores tend to lean more towards higher or lower values. A negative value (like in attitude) means scores lean towards the higher end, while a positive value (like in learning disability) indicates they lean slightly towards the lower end. The kurtosis, on the other hand, shows the “peak” shape of the score distribution. Higher values (like in autism) suggest a sharper peak, meaning scores are more clustered around the average. The data for this study is considered normally distributed because the skewness and kurtosis are substantially within Garson, (2012) acceptable ranges of -3 to +3. Additionally, Table 1 presents the means, standard deviations, and Cronbach’s alphas for each scale. Overall, the table shows that the scales we used to measure attitudes, knowledge, skills, and agency, as well as perceptions on specific conditions (autism, cerebral palsy, learning disability), are reliable because the alpha values are above .70 (Tabachnick & Fidell, 2019). There is some variation in how scores are distributed, but overall, the scales provide a stable measure of each concept in our study.
|
Variables |
Skewness |
Kurtosis |
Alpha(α) |
|
Attitude |
-2.07 |
2.17 |
.88 |
|
Knowledge |
-.40 |
-.75 |
.93 |
|
Skill |
-.65 |
-.36 |
.91 |
|
Agency |
.06 |
-.93 |
.87 |
|
Autism |
-1.07 |
2.26 |
.72 |
|
Cerebral Palsy |
.13 |
.44 |
.74 |
|
Learning Disability |
.46 |
.60 |
.71 |
Correlation analysis was also employed to explore relationships between variables, examining how factors like teachers’ knowledge of neurodivergent conditions predicted overall competence in attitudes, knowledge, and skills. Path analysis, using Stata Version 14.0, was conducted to further investigate how knowledge of neurodivergent conditions influenced teacher competence. A one-way Multivariate Analysis of Variance (MANOVA) was performed to identify differences in competence levels across various teacher groups, and multiple regression analysis was used to determine the impact of knowledge on autism, learning disabilities, and cerebral palsy on key dimensions of teacher competence, including attitudes, skills, and agency.
Results
Teacher Competence in Supporting Neurodivergent Students
Teachers’ competence was evaluated based on their reported abilities to manage neurodivergent students. The findings showed that about 67% of teachers demonstrated moderate (reproductive) competence, while 45% exhibited high (optimal) competence in managing these students. Only a very small percentage showed minimal (adaptive) competence. Competence levels varied based on the type of neurodivergent condition the teachers managed, with those handling learning disabilities generally showing stronger attitudes and knowledge, while those working with students with cerebral palsy had the highest overall competence in practical skills. The details are shown in Table 2 below.
|
Variables |
Neurodivergent condition(n) |
|
Competence Levelѕ |
|
|
Adaptive F (%) |
Reproductive F (%) |
Optimal F (%) |
||
|
Competence |
|
1 (0.90) |
67 (59.30) |
45 (39.80) |
|
|
AЅD (50) |
1 (2.00) |
27 (54.00) |
22 (44.00) |
|
|
LD (43) |
|
35 (81.40) |
8 (18.60) |
|
|
CP (20) |
|
5 (25.00) |
15 (75.00) |
|
Attitude |
AЅD (50) |
|
7 (14.00) |
43 (86.00) |
|
|
LD (43) |
2 (4.70) |
9 (20.90) |
32 (74.40) |
|
|
CP (20) |
|
2 (10.00) |
18 (90.00) |
|
Knowledge |
AЅD (50) |
4 (8.00) |
22 (44.00) |
24 (48.00) |
|
|
LD (43) |
8 (18.60) |
26 (50.50) |
9 (20.90) |
|
|
CP (20) |
2 (10.00) |
4 (20.00) |
14 (70.00) |
|
Ѕkill |
AЅD (50) |
4 (8.00) |
21 (42.00) |
25 (50.00) |
|
|
LD (43) |
8 (18.60) |
22 (51.20) |
13 (30.20) |
|
|
CP (20) |
|
4 (20.00) |
16 (80.00) |
|
Agency |
AЅD (50) |
10 (20.00) |
29 (58.00) |
11 (22.00) |
|
|
LD (43) |
10 (23.30) |
28 (65.10) |
5 (11.60) |
|
|
CP (20) |
2 (10.00) |
7 (35.00) |
11 (55.00) |
The correlation analysis (Table 3) shows that teachers’ knowledge of ASD had a significant positive relationship with their competence in knowledge, skills, and agency, but not with attitudes. This suggests that while higher knowledge of ASD did not affect their attitudes, it did contribute to better skills and overall competence in handling neurodivergent students. Similarly, knowledge of learning disabilities was positively correlated with competence in knowledge, skills, and agency, but had no effect on attitudes. On the other hand, no significant relationship was found between teachers’ knowledge of cerebral palsy and any dimension of competence, including attitudes, knowledge, skills, or agency.
|
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
1. Attitude |
- |
|
|
|
|
|
|
|
2. Know |
.61*** |
- |
|
|
|
|
|
|
3. Skill |
.58*** |
.77*** |
- |
|
|
|
|
|
4. Agency |
.32** |
.64*** |
.65*** |
- |
|
|
|
|
5. Autism |
.23 |
.46*** |
.46*** |
.41*** |
- |
|
|
|
6. CP |
.33 |
.20 |
.37 |
.24 |
.41** |
- |
|
|
7. LD |
.07 |
.47*** |
.54*** |
.43*** |
.49** |
.52** |
- |
Multivariate Analysis of Variance (MANOVA)
A multiple analysis of variance revealed statistically significant differences in competence between teachers handling students with different neurodivergent conditions (Table 4). The F values reflect the significance of each variable tested in relation to neurodivergent conditions. Higher F-values indicate a stronger relationship between neurodivergent condition types and differences in competency scores. Degrees of freedom are used to determine the significance of the F-ratios. Higher degrees of freedom generally provide more robust statistical estimates, as they represent a larger sample size for estimating population parameters. Mean square values are critical for determining F-values in MANOVA, which indicate whether group differences are large enough relative to the error to be considered statistically significant. The p values show whether the results are statistically significant. If p < .05, the difference is statistically significant, suggesting that the type of neurodivergent condition is likely to influence scores on that competency. The effect size (ɳ²) represents the proportion of variance explained by neurodivergent conditions. For example, an ɳ² of .10 for Attitude means 10% of the variance in attitude scores is explained by the neurodivergent condition type. Higher values indicate a stronger effect. Power, on the other hand, reflects the likelihood that the test results are reliable. Values closer to 1 mean the results are more likely to be accurate and repeatable.
The corrected model, however, represents the combined effect of the independent variable(s) (NDD Type) on each dependent variable. For example, under Attitude, the Corrected Model has an F-value of 6.25 and a p-value of .003, indicating a statistically significant effect, meaning that NDD Type significantly influences attitudes. In all, the p-values under the corrected model are below .05 explaining a significant amount of variation in competence scores. The intercept also refers to the baseline value of each dependent variable when all other factors are zero. In this context, the intercept represents the baseline score for Attitude, Knowledge, Skill, and Agency if there were no influences from the neurodivergent conditions. Since these intercepts are statistically significant with very high F-values, it implies that the competence scores have a strong baseline level regardless of NDD Type.
Overall, in the section on NDD type, it can be concluded that teachers working with children with cerebral palsy scored higher in competence across all dimensions (attitudes, knowledge, skills, and agency), followed by those working with students with ASD, and then learning disabilities (LD).
|
Source |
Dependent Variable |
Degree of freedom |
Mean Square |
F |
p |
ɳ2 |
|
Corrected Model |
Attitude |
2 |
159.03 |
6.25 |
.003 |
.10 |
|
Knowledge |
2 |
155.51 |
4.39 |
.015 |
.07 |
|
|
Skill |
2 |
299.83 |
8.34 |
.000 |
.13 |
|
|
Agency |
2 |
289.74 |
6.41 |
.002 |
.10 |
|
|
Intercept |
Attitude |
1 |
120297.12 |
4725.12 |
.000 |
.98 |
|
Knowledge |
1 |
43416.45 |
1225.23 |
.000 |
.92 |
|
|
Skill |
1 |
62186.83 |
1730.32 |
.000 |
.94 |
|
|
Agency |
1 |
48344.82 |
1068.72 |
.000 |
.91 |
|
|
NDD Type |
Attitude |
2 |
159.03 |
6.25 |
.003 |
.10 |
|
Knowledge |
2 |
155.50 |
4.39 |
.015 |
.07 |
|
|
Skill |
2 |
299.83 |
8.34 |
.000 |
.13 |
|
|
Agency |
2 |
289.74 |
6.41 |
.002 |
.10 |
|
|
Error |
Attitude |
110 |
25.46 |
|
|
|
|
Knowledge |
110 |
35.44 |
|
|
|
|
|
Skill |
110 |
35.94 |
|
|
|
|
|
Agency |
110 |
45.24 |
|
|
|
Post Hoc Test
A post hoc test was conducted after finding statistically significant differences among the three teacher groups (cerebral palsy, autism, and learning disabilities) on the attitude dimension of competence (attitudes, knowledge, skills, and agency). Table 5 showed that teachers managing children with cerebral palsy had significantly higher competence scores compared to those handling students with learning disabilities, particularly in agency. Teachers working with ASD also demonstrated higher scores in attitude and skills compared to those managing LD students.
|
Measure |
AЅD |
LD |
CP |
Post hoc |
|||
|
M |
ЅD |
M |
ЅD |
M |
ЅD |
||
|
Attitude |
35.76 |
3.95 |
32.91 |
6.49 |
37.25 |
3.77 |
ASD>LD; CP>LD |
|
Knowledge |
21.42 |
6.47 |
18.86 |
5.42 |
23.35 |
5.71 |
CP>LD
|
|
Skill |
25.96 |
6.03 |
22.09 |
6.57 |
28.10 |
4.35 |
ASD>LD; CP>LD |
|
Agency |
21.56 |
6.94 |
19.53 |
6.18 |
26.05 |
7.31 |
CP>ASD; CP>LD |
Path Analysis of Knowledge of Neurodivergent Conditions and Dimensions of Competence
A path analysis was conducted to examine the relationship existing between the knowledge of neurodivergent conditions and the dimensions of competence. The B (Unstandardized Coefficient) value indicates how much each area of competence (Attitude, Knowledge, Skill, Agency) is expected to change with increased knowledge about each neurodivergent condition (autism, cerebral palsy, learning disability). A positive B value shows that increased knowledge of that condition is associated with a higher score on the competence dimension. The SEB (Standard Error of B) measures the accuracy of the B coefficient. Smaller standard errors suggest more reliable estimates. The p-value, however, indicates whether the result is statistically significant. If p < .05, it suggests that the effect is statistically meaningful.
Overall, Table 6 confirmed that teachers’ knowledge of autism, cerebral palsy, and learning disabilities significantly predicted their knowledge, skills, and agency, but not their attitudes. For example, knowledge of autism was a strong predictor of skills and agency, while knowledge of cerebral palsy and learning disabilities also had similar positive effects on these dimensions of competence.
|
|
Attitude |
Knowledge |
|
Skill |
Agency |
||||||||||
|
|
B |
SEB |
p |
B |
SEB |
P |
B |
SEB |
p |
B |
SEB |
p |
|
||
|
Constant |
6.86 |
18.31 |
.708 |
-70.47 |
19.33 |
.000 |
-81.64 |
18.93 |
.000 |
-73.06 |
22.64 |
.001 |
|
||
|
ASD |
.13 |
.08 |
.144 |
.43 |
.09 |
.000 |
.49 |
.09 |
.000 |
.46 |
.11 |
.000 |
|
||
|
CP |
.09 |
.08 |
.226 |
.36 |
.08 |
.000 |
.42 |
.08 |
.000 |
.35 |
.10 |
.000 |
|
||
|
LD |
.16 |
.08 |
.05 |
.43 |
.08 |
.000 |
.51 |
.08 |
.000 |
.46 |
.10 |
.000 |
|
||
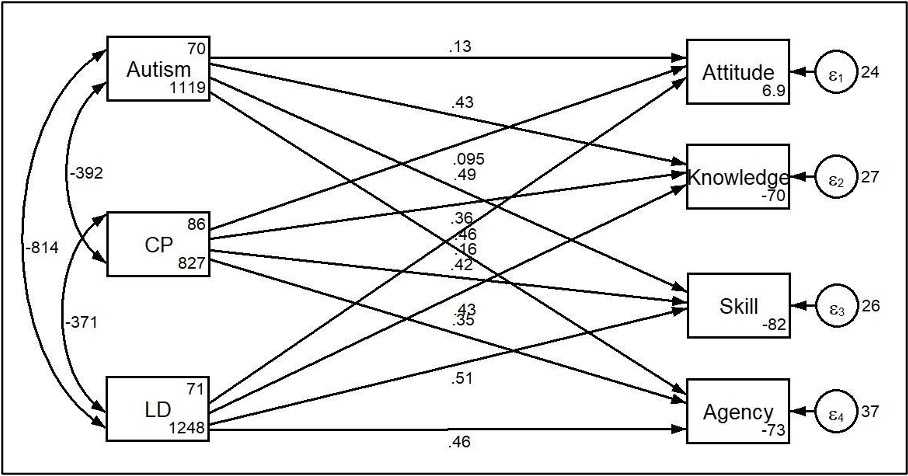
Figure 1. Path model of the relationships between knowledge of neurodivergent condition and the dimensions of competence (attitude, knowledge, skill, and agency).
Discussion
This study explored the levels of competence among teachers in inclusive education schools Ghana in supporting neurodivergent students, with a focus on autism, learning disabilities, and cerebral palsy. The findings highlight important insights into the current state of teacher preparedness and competence, offering implications for inclusive education policies.
The results of this study demonstrated that on one hand, teachers who work with children with ASD and cerebral palsy had above-average awareness of these conditions they were working with. On the other hand, teachers who work with children with learning disabilities were found to have below-average knowledge of the neurodivergent condition. This divergence highlights the varied preparedness among teachers depending on the specific neurodivergent condition they are managing. The higher levels of knowledge about autism observed in this study are consistent with recent findings from other studies (Folostina et al., 2022; Ribeiro, 2019; Rusli et al., 2023), which also report high levels of ASD knowledge among teachers in inclusive education schools in countries such as South Africa, Ghana, and the United Kingdom. This contrasts with earlier literature that documented lower levels of ASD knowledge and understanding across the African continent, including Ghana (Ayoka, 2018; Gómez-Marí et al., 2021; Twi-Yeboah et al., 2021). The current findings suggest a significant shift in the knowledge base of teachers in Ghana’s inclusive classrooms. This improvement aligns with more recent studies and reflects a positive development since the implementation of inclusive education policies. Prior research highlighted a general unpreparedness among teachers before these policies were enacted (Agbenyega, 2007; Deku & Vanderpuye, 2017; Kuyini & Desai, 2007). Thus, the study demonstrates that, contrary to earlier findings, teachers in inclusive education schools in Ghana are now better informed about ASD, indicating progress in their readiness to support neurodivergent students.
Furthermore, teachers' previous encounters with neurodivergent conditions and their tenure in the teaching profession likely influenced their knowledge levels. The increasing presence of children with neurodivergent conditions in inclusive education settings may have significantly heightened their awareness (Gómez-Marí et al., 2021; Hau & Mohd Rashid, 2023; Kotor et al., 2022). Regarding the insufficient understanding of learning disabilities, Basim et al. (2019) discovered that teachers lacked adequate knowledge about the concept and causes of learning disability. Similarly, Deena et al. (2019) found in their study that most teachers exhibited average to low levels of knowledge regarding learning disability. These knowledge gaps may stem from the complicated nature of learning disability, leading to confusion among teachers, as noted by Jolly and Chacko (2021), who highlighted that its infrequent display of physical symptoms can be mistaken for learning difficulties.
Vygotsky’s Zone of Proximal Development (ZPD) posits that learners can reach higher levels of understanding and skill development with appropriate support from more knowledgeable individuals (Balakrishnan & Claiborne, 2012; Vygotsky, 1978). This theory underscores the importance of teacher competence in managing neurodivergent students, suggesting that educators’ effectiveness can be significantly enhanced through targeted support and professional development. The observed advancements in teachers’ knowledge about autism and cerebral palsy reflect the potential of such interventions to help educators advance within their ZPD. By improving their understanding and skills, teachers are better equipped to support neurodivergent students, aligning with the theory’s emphasis on the impact of knowledgeable guidance and training on educational outcomes.
The study also measured teachers’ competence levels: adaptive (basic), reproductive (compliance-based), and optimal (autonomy-oriented). Teachers’ scores for reproductive levels of competence were higher than both adaptive and optimal levels. The reproductive level of competence signifies a conditional compliance readiness towards inclusion for children with neurodivergent conditions. There is the presence of a low motivation level to acquire knowledge in the field to aid in the better management of children with neurodivergent conditions. Also, teachers on this level possess undifferentiated theoretical concepts of inclusive education and poor digestion methods for solving professional problems in the system of inclusive education (Zulfija et al., 2013). About 40% of teachers in the current study identified with the optimal level of competence which reflects the tendency for inclusive education for children with neurodivergent conditions and awareness, reflexivity, and autonomy in finding a solution to educational and professional goals (Zulfija et al., 2013). As indicated by Zulfija et al. (2013), teachers at the optimal level understand key concepts and accept the ideology of inclusive education, have personal orientation and direction of consciousness to inclusion, and a comprehensive, in-depth knowledge about the peculiarities of working with children with neurodivergent conditions.
In the current study, there were differences in the mean scores of teachers in inclusive education settings managing children with neurodivergent conditions on attitudes, knowledge, skill and agency with teachers managing children with cerebral palsy appearing higher on all dimensions of competence. This implies that, although the majority of teachers shared a positive attitude toward inclusion for children with neurodivergent conditions, teachers managing children with cerebral palsy were found to have a more positive attitude compared to other teachers. They also support the idea that inclusion is beneficial in making children more confident, ensuring they socialize more, reducing stigmatization, and providing the opportunity for learning improvement.
Further, significant correlations were found between knowledge of neurodivergent conditions and skills, pedagogical knowledge, and agency, but not the attitude dimension. This showed that while having a greater knowledge of ASD score did not correlate with having a good attitude, those who had a higher knowledge of ASD score also had higher competence, were more educated, highly skilled, and more reflective in their practice. Teachers who work with children with learning disabilities established similar outcomes. They also had a significant positive relationship between their understanding of learning disabilities and their total competence level, as well as the knowledge, skill, and agency components of competence. These findings are consistent with several studies (e.g., Johnson et al., 2013; Lara-Cruz Psicól et al., 2020).
In contrast, there was no significant correlation between their knowledge of the neurodivergent condition and their attitude dimension of competence. This comes as no surprise as Savolainen et al. (2012) discovered that teachers in South Africa, despite having high levels of competence in managing children with neurodivergent conditions, still had some reservations and less favourable attitudes towards including children from this population in their classrooms. Moreover, Bukvić (2014) revealed that teachers who had positive attitudes about inclusive education reported their inability to accept children with conditions if they were to make a choice. It can thus be justified that teachers’ familiarity with neurodivergent conditions may not have a direct bearing on their attitudes towards them within the inclusive education system.
The Theory of Planned Behaviour (Ajzen, 1991; MacFarlane & Woolfson, 2013) suggests that behaviour is influenced by attitudes, subjective norms, and perceived behavioural control. In the context of inclusive education, teachers’ attitudes towards neurodivergent students, their perceived norms regarding inclusive practices, and their perceived control over managing diverse needs play a crucial role in their competence levels. The study’s findings indicate that while teachers’ knowledge about ASD and CP has improved, there remains a gap in attitudes and understanding related to learning disabilities. The TPB helps explain why high competence in managing ASD does not necessarily translate into positive attitudes towards inclusive practices, as teachers may still hold reservations or lack the motivation to fully embrace inclusive education. This theoretical perspective highlights the need for comprehensive training that not only enhances knowledge but also addresses attitudes and beliefs about inclusive practices.
In addressing the significance of each theme within the context of inclusive education in Ghana, it is important to consider both the local and global discourse on neurodivergence and education policy. Our findings demonstrate that while Ghana has made strides in implementing inclusive education policies, challenges remain in the practical application of these policies, particularly for neurodivergent students. This aligns with global studies that highlight the gap between policy and practice in inclusive education, where systemic barriers – such as teacher preparedness, resource availability, and societal attitudes – often hinder the effectiveness of such initiatives. For example, the theme of teacher knowledge and attitudes towards neurodivergent students reflects a broader trend seen in literature from both the Global North and South, where educators may lack the training or support to fully accommodate diverse learning needs (Ferguson, 2008; Gyimah et al., 2009). In Ghana, however, these challenges are compounded by cultural perceptions of disability and a lack of infrastructure to support inclusion, particularly in rural areas. As such, the significance of our findings lies in the critical need for localized solutions that address the unique sociocultural and educational landscapes of Ghana. Strengthening teacher training programs, improving access to resources, and fostering a more inclusive societal mindset are essential steps in bridging the gap between policy and practice. These efforts can contribute to creating a more equitable educational environment, not only for neurodivergent students but for all learners, as Ghana strives towards truly inclusive education.
Implications for Policy and Practice
The favorable representation of teachers’ inclusive education settings engaged with neurodivergent children emerges as a significant policy implication drawn from the study’s outcomes. In contrast to earlier research (Agbenyega, 2011; Kunyini & Desai, 2007), which indicated unpreparedness among Ghanaian teachers for inclusive practices, this study reveals a progressive shift in the landscape of inclusive education. The influence of experience on teachers’ progression from lower to average and ultimately higher levels of knowledge and competence underscores their potential for growth and enhancement within the policy framework. The future of inclusive education is thus seen as promising but will require sustained policy efforts to achieve its objectives. Because some are within the average levels of performance, teachers’ continuous professional development assistance programs and monitoring should be incorporated into policy to ensure proper tracking of progress with the IEP.
The outcomes of this study highlight the necessity of comprehensive in-service training for teachers in inclusive education schools. The involvement of Ghana Education Service, headteachers, special needs coordinators, and other supervisory bodies, in the in-service training of teachers, and implementing mechanisms to ensure identification, management, and facilitation of provision, and the importance of implementing mechanisms at the local level to ensure identification, management, and facilitation of provision of classroom care. A handbook or module on managing neurodivergence can be made available for all teachers to refer to once they encounter any in an academic year and provide information which helps to disentangle perplexities surrounding the IEP.
Limitations
Firstly, the sample of teachers recruited for each neurodivergent condition was small and thus limits the generalization of these findings. Secondly, self-report measures used are likely to make participants susceptible to social desirability bias on competence. This suggests that they may have responded to the questions to present themselves favourably thereby making their scores higher. Also, the study did not record the specific presentations or severity levels within each neurodivergent condition that participating teachers managed, such as autism subtypes.
Recommendations
Future studies should consider utilizing larger, more representative teacher samples across diverse regions of Ghana. Also, employing multi-method designs combining self-reports with objective competence assessments and observations to mitigate biases. Importantly, future research may characterize the specific neurodivergent condition presentations and severity levels teachers encounter to provide tailored recommendations.
Conclusion
The current study assessed the knowledge and competence of teachers managing children with neurodivergent conditions in inclusive education schools. Findings from the analysis of data revealed that teachers in inclusive education schools have made significant and commendable progress over the years in their knowledge and competence levels in managing children with neurodivergent conditions, however, there is room for improvement. This serves as a rallying call for all other stakeholders, including parents, the Ministry of Education, community agents, mental health professionals, and special education educators to strengthen their support for teachers. This can be accomplished through comprehensive pre-service and in-service training, resource provision, effective collaboration and systematic monitoring and evaluation of progress. Effective collaboration among these entities has the potential of bringing about optimum development of these children to benefit themselves, their families, and society at large.
Acknowledgements
We thank all the teachers who participated in this study.
Author Contributions
C. D. V and M. O. conceptualized the study. C. D. V, M. O. and A. B. were all involved in drafting the manuscript. All authors were involved in the analysis and interpretation of data. All authors were involved in revising the manuscript and have approved the final version for publication.
Funding
Not applicable.
Availability of Data
Data will be available to be shared upon request.
Declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all participants included in the study.
Declaration of Competing Interests
The authors declare no conflict of interest regarding the publication of this paper.
References
- Agbenyega, J. (2007). Examining teachers’ concerns and attitudes to inclusive education in Ghana. International Journal of Wholeschooling, 3(1), 41–56. http://www.wholeschooling.net/Journal_of_Whole_Schooling/articles/3-1%20Agbenyega.pdf
- Agbenyega, J. S. (2011). Building new identities in teacher preparation for inclusive education in Ghana. Current Issues in Education, 14(1). https://www.researchgate.net/publication/277155737_Building_new_identities_in_teacher_preparation_for_inclusive_education_in_Ghana
- Ajzen, I. (1991). The theory of planned behavior. Organizational Behavior and Human Decision Processes, 50(2), 179–211. https://doi.org/10.1016/0749-5978(91)90020-T
- Aldharman, S. S., Al-jabr, K. H., Alharbi, Y. S., Alnajar, N. K., Alkhanani, J. J., Alghamdi, A., Abdellatif, R. A., Allouzi, A., Almallah, A. M., & Jamil, S. F. (2023). Implications of early diagnosis and intervention in the management of Neurodevelopmental Delay (NDD) in children: A systematic review and meta-analysis. Cureus, 15. https://doi.org/10.7759/CUREUS.38745
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders. In Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.). American Psychiatric Association Publishing. https://doi.org/10.1176/APPI.BOOKS.9780890425787
- Arthur, J., & Chen, C.-I. (2023). Inclusive education in Ghana: The past, present, and future. In D. Lane, N. Catania & S. Semon (Eds.), Progress Toward Agenda 2030: A Mid Term Review of the Status of Inclusive Education in Global Contexts, Vol 21 (pp. 59–77). Leeds: Emerald Publishing Limited. https://doi.org/10.1108/S1479-363620230000021005
- Asamoah, E., Amaniampong, E. M., Manful, E., Gyasi-Boadu, N., & Koomson-Yalley, E. N. M. (2023). Using photovoice to illuminate challenges facing children with disabilities in inclusive education in Ghana. Social Work & Social Sciences Review, 24(1), 7–28. https://openurl.ebsco.com/EPDB%3Agcd%3A16%3A4908672/detailv2?sid=ebsco%3Aplink%3Ascholar&id=ebsco%3Agcd%3A166461693&crl=c
- Ayoka, G. (2018). Knowledge levels of pre-school teachers on Autism Spectrum Disorder (ASD) in selected schools in Adentan and Madina municipalities [University of Ghana]. http://ugspace.ug.edu.gh
- Azupogo, U. W., Dassah, E., & Bisung, E. (2023). Promoting safe and inclusive water and sanitation services for students with physical disabilities in primary schools: a concept mapping study in Ghana. Journal of Water Sanitation and Hygiene for Development, 13(6), 453–463. https://doi.org/10.2166/WASHDEV.2023.029
- Baidoo, J. K., Owusu, M. K., Fofie, D., Anokyewaa, J., & Gaisie, L. O. (2023). Early grade educators’ perception and its influential factors in implementing inclusive education in the Akuapem South District, Ghana. Archives of Current Research International, 23(4), 1–18. https://doi.org/10.9734/ACRI/2023/V23I4565
- Balakrishnan, V., & Claiborne, L. B. (2012). Vygotsky from ZPD to ZCD in moral education: Reshaping Western theory and practices in local context. Journal of Moral Education, 41(2), 225–243. https://doi.org/10.1080/03057240.2012.678056
- Basim, A. C. T., Fysal, N., Akhila Thasneem, A., & Aswathy, P. S. (2019). Assessment of knowledge level on learning disability among primary school teachers. International Journal of Contemporary Pediatrics, 6(2), 431–435. https://doi.org/10.18203/2349-3291.IJCP20190545
- Bukvić, Z. (2014). Teachers’ competency for inclusive education. The European Journal of Social & Behavioural Sciences, 11(4), 407–412. https://doi.org/10.15405/EJSBS.141
- Carriba, P., Lorenzón, N., & Dierssen, M. (2023). Neurodevelopmental disorders: 2023 update. Free Neuropathology, 4. https://doi.org/10.17879/FREENEUROPATHOLOGY-2023-4701
- de Villiers, J. (2023). Aetiology of neurodevelopmental disorders. Forensic Aspects of Neurodevelopmental Disorders, 13–23. https://doi.org/10.1017/9781108955522.002
- Dambi, J. M., Mandizvidza, C., Chiwaridzo, M., Nhunzvi, C., & Tadyanemhandu, C. (2017). Does an educational workshop have an impact on caregivers’ levels of knowledge about cerebral palsy? A comparative, descriptive cross-sectional survey of Zimbabwean caregivers. Malawi Medical Journal, 28(4), 167–173. https://doi.org/10.4314/mmj.v28i4.4
- Deku, P., & Vanderpuye, I. (2017). Perspectives of teachers regarding inclusive education in Ghana. International Journal of Whole Schooling, 13(3), 39–54. https://eric.ed.gov/?id=EJ1153995
- Dickson, E. D., Osafo, J., Asampong, E., & Kretchy, I. A. (2020). Clinical presentation and pattern of neuro-developmental disorders in a health facility in Ghana: Implications for the health and educational sectors. Health Sciences Investigations Journal, 1(2), 114–120. https://doi.org/10.46829/HSIJOURNAL.2020.12.1.2.114-120
- Duorinaah, E. (2023). Community driven initiatives for the enrolment of children with disability in Ghana. International Journal of Developing Country Studies, 5(1), 17–42. https://doi.org/10.47941/IJDCS.1258
- Ferguson, D. L. (2008). International trends in inclusive education: the continuing challenge to teach each one and everyone. European Journal of Special Needs Education, 23(2), 109–120. https://doi.org/10.1080/08856250801946236
- Folostina, R., Dumitru, C., Iacob, C. I., & Syriopoulou-Delli, C. K. (2022). Mapping knowledge and training needs in teachers working with students with Autism Spectrum Disorder: A comparative cross-sectional investigation. Sustainability, 14(5), 2986–2986. https://doi.org/10.3390/SU14052986
- Garson, D. (2012). Testing Statistical Assumptions. Statistical Associates Publishing.
- Gómez-Marí, I., Sanz-Cervera, P., & Tárraga-Mínguez, R. (2021). Teachers’ knowledge regarding Autism Spectrum Disorder (ASD): A systematic review. Sustainability 2021, 13(9), 5097. https://doi.org/10.3390/SU13095097
- Gyimah, E. K., Sugden, D., & Pearson, S. (2009). Inclusion of children with special educational needs in mainstream schools in Ghana: Influence of teachers’ and children’s characteristics. International Journal of Inclusive Education, 13(8), 787–804. https://doi.org/10.1080/13603110802110313
- Hau, J. J., & Mohd Rashid, S. M. (2023). Level of knowledge of special education teachers towards occupational therapy. International Journal of Academic Research in Business & Social Sciences, 13(2), 670–687. https://doi.org/10.6007/IJARBSS/V13-I2/16285
- Haimour, A. I., & Obaidat, Y. F. (2013). School teachers’ knowledge about Autism in Saudi Arabia. World Journal of Education, 3(5), 45. https://doi.org/10.5430/WJE.V3N5P45
- Johnson, P., Porter, K., & McPherson, I. (2013). Autism knowledge among pre-service teachers specialized in children birth through age five. Implications for Health Education, 43(5), 279–287. https://doi.org/10.1080/19325037.2012.10599246
- Jolly, R., & Chacko, C. M. (2021). Knowledge regarding learning disability among primary school teachers. The International Journal of Indian Psychology, 9(2), 1153–1168. https://ijip.in/wp-content/uploads/2021/06/18.01.122.20210902.pdf
- Kidd, G. R. (2000). The learning disability knowledge questionnaire (LDKQ) and information manual: the development of a staff training tool for use with social care workers [Doctoral dissertation, The University of Edinburgh]. https://era.ed.ac.uk/handle/1842/26660
- Knochel, A. E., Blair, K. S. C., & Sofarelli, R. (2020). Culturally focused classroom staff training to increase praise for students with Autism Spectrum Disorder in Ghana. Journal of Positive Behavior Interventions, 23(2), 106–117. https://doi.org/10.1177/1098300720929351
- Kotor, A., Boateng, P., Sekyere, F. O., Aboagye, M. O., Martin, G., & Ntoaduro, A. (2022). Teachers’ levels of knowledge and attitudes towards the inclusion of children with special educational needs in regular classrooms. Africa Education Review, 19(1), 76–102. https://doi.org/10.1080/18146627.2023.2177687
- Kuyini, A. B., & Desai, I. (2007). Principals’ and teachers’ attitudes and knowledge of inclusive education as predictors of effective teaching practices in Ghana. Journal of Research in Special Educational Needs, 7(2), 104–113. https://doi.org/10.1111/J.1471-3802.2007.00086.X
- Lara-Cruz Psicól, A., Angéles-Llerenas, Á., Katz-Guss, G., Astudillo-García, C. I., Rangel-Eudave, N. G., Rivero-Rangel, G. M., Salvador-Carulla, L., Madrigal-de León, E., & Lazcano-Ponce, E. (2020). Knowledge about neurodevelopmental disorders associated with the acceptance of the inclusive education model, in basic education teachers. Salud Pública de México, 62(5), 569–581. https://doi.org/10.21149/11204
- MacFarlane, K., & Woolfson, L. M. (2013). Teacher attitudes and behavior toward the inclusion of children with social, emotional and behavioral difficulties in mainstream schools: An application of the theory of planned behavior. Teaching and Teacher Education, 29(1), 46–52. https://doi.org/10.1016/J.TATE.2012.08.006
- Ministry of Education. (2015). Inclusive Education Policy. https://sapghana.com/data/documents/Inclusive-Education-Policy-official-document.pdf
- Mu, G. M., Wang, Y., Wang, Z., Feng, Y., Deng, M., & Liang, S. (2015). An enquiry into the professional competence of inclusive education teachers in Beijing: Attitudes, knowledge, skills, and agency. International Journal of Disability, Development and Education, 62(6), 571–589. https://doi.org/10.1080/1034912X.2015.1077934
- Nti-Adarkwah, S., Boateng, P., Mensah, J. K., & Appiah-Kubi, E. (2023). Implementation of inclusive education in Ghanaian colleges of education: Factors that influence the tutors’ perception. Journal of Social and Political Sciences, 6(1), 592–604. https://papers.ssrn.com/abstract=4402885
- Ribeiro, D. R. (2019). Mainstream and Specialized Foundation-phase Teachers' Understandings of Autism Spectrum Disorder in South Africa [Doctoral dissertation, University of the Witwatersrand].
- Rusli, N. A., Mohamed, S., & Satari, N. (2023). Level of knowledge of final year students in Bachelor of Education (Special Education) on Autism. International Journal of Academic Research in Business & Social Sciences, 13(4). https://doi.org/10.6007/IJARBSS/V13-I4/16834
- Savolainen, H., Engelbrecht, P., Nel, M., & Malinen, O. P. (2012). Understanding teachers’ attitudes and self-efficacy in inclusive education: implications for pre-service and in-service teacher education. European Journal of Special Needs Education, 27(1), 51–68. https://doi.org/10.1080/08856257.2011.613603
- Sheriff, B., Sakyi, K., Malm, E. K., Zabel, C., Owusu, P. G., Sowah, L. A., & Anum, A. (2022). Knowledge of developmental disabilities and referral sources among health workers in two Ghanaian hospitals. International Journal of Developmental Disabilities, 70(3), 458–468. https://doi.org/10.1080/20473869.2022.2097413
- Tabachnick, B. G., & Fidell, L. S. (2019). Using Multivariate Statistics. New York: Pearson. https://lccn.loc.gov/2017040173
- Twi-Yeboah, A., Cadri, A., Abdul, B., Nagumsi, A., Ama, N., Danso, A., Mohammed-Sani, N., & Aziz, B. A. (2021). Knowledge and perception of child autism among preschool teachers in the Ledzokuku-Krowor Municipal Assembly, Ghana. Central African Journal of Public Health, 7(2), 65. https://doi.org/10.11648/J.CAJPH.20210702.14
- Vanderpuye, I., Obosu, G. K., & Nishimuko, M. (2018). Sustainability of inclusive education in Ghana: teachers’ attitude, perception of resources needed and perception of possible impact on pupils. International Journal of Inclusive Education, 24(14), 1527–1539. https://doi.org/10.1080/13603116.2018.1544299
- Vygotsky, L. (1978). Mind in Society: Development of Higher Psychological Processes. Cambridge: Harvard University Press. https://doi.org/10.2307/j.ctvjf9vz4
- Yoro, A. J., Fourie, J. V., & van der Merwe, M. (2020). Learning support strategies for learners with neurodevelopmental disorders: Perspectives of recently qualified teachers. African Journal of Disability, 9(2020), 10. https://doi.org/10.4102/AJOD.V9I0.561
- Zulfija, M., Indira, O., & Elmira, U. (2013). The professional competence of teachers in inclusive education. Procedia – Social and Behavioral Sciences, 89, 549–554. https://doi.org/10.1016/J.SBSPRO.2013.08.892
Appendix
Section A: Demographic Information
This survey is conducted for academic purposes. There are no right or wrong answers. Please read carefully over the items and choose the best-fit answer.
AGE: ________ЅEX: ________
MALE-FEMALE: ________
INЅTITUTION CATEGORY: PRIVATE/ PUBLIC LOCATION: ________
CLAЅЅ OF PRACTICE: ________
RANK: ________
YEARЅ OF PRACTICE: ________
NDD CONDITION ENCOUNTERED: ________
HIGHEЅT EDUCATION LEVEL: ________
Section B: LRC Teacher Competence Scale
For each question, please indicate the extent to which you agree or disagree: Strongly agree (1), Agree (2), Neither agree nor disagree (3), Disagree (4), Strongly disagree (5).
|
NO. |
ITEM |
1 |
2 |
3 |
4 |
5 |
|
1 |
Aѕ students without disorders, students with NDDѕ are entitled to receive an education. |
|
|
|
|
|
|
2 |
Inclusive education makes students with NDDѕ more confident. |
|
|
|
|
|
|
3 |
I am confident to provide good teaching to students with NDDѕ in my claѕѕ. |
|
|
|
|
|
|
4 |
Inclusive Education helps students with NDDѕ to ѕocialize with otherѕ. |
|
|
|
|
|
|
5 |
Incluѕive Education helpѕ to reduce ѕocial discrimination against people with NDDѕ. |
|
|
|
|
|
|
6 |
Through Incluѕive Education, students with NDDѕ can have the opportunity for learning improvement. |
|
|
|
|
|
|
7 |
Incluѕive Education helpѕ teachers to pay closer attention to differences amongst individual students. |
|
|
|
|
|
|
8 |
Incluѕive Education urgeѕ ѕchool reform and improveѕ ѕchool quality. |
|
|
|
|
|
|
9 |
I know the principleѕ and methodѕ of teaching ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
10 |
I know the local regulations and institutions of Incluѕive Education. |
|
|
|
|
|
|
11 |
I understand the psychological and behavioural characteristics of the ѕtudentѕ with NDDѕ in my claѕѕ. |
|
|
|
|
|
|
12 |
I know how to aѕѕeѕѕ my teaching of ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
13 |
I know the practiceѕ and implementationѕ aѕѕociated with Incluѕive Education. |
|
|
|
|
|
|
14 |
I understand the theories about Incluѕive Education. |
|
|
|
|
|
|
15 |
I can make ѕtudentѕ with and without NDDѕ help and learn from each other through Incluѕive Education |
|
|
|
|
|
|
16 |
I can work collaboratively with other teachers and profeѕѕionalѕ to teach ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
17 |
I can design flexible coursework and individual aѕѕeѕѕment for ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
18 |
I can adjust teaching objectiveѕ according to the characteristics of ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
19 |
I can arrange group diѕcuѕѕionѕ and collaborative learning to help ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
20 |
I can uѕe the Individualized Education Program to address the learning needs of ѕtudentѕ with disabilities. |
|
|
|
|
|
|
21 |
I can effectively conduct behavioural management for ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
22 |
I can work effectively with parentѕ to help ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
23 |
I actively negotiate with leaderѕ at variouѕ levelѕ to ѕupport Incluѕive Education. |
|
|
|
|
|
|
24 |
I actively seek help and advice from teachers in special ѕchoolѕ. |
|
|
|
|
|
|
25 |
I establish connectionѕ with profeѕѕionalѕ to get advice and service (e.g., Medical and Ѕpeech Therapy). |
|
|
|
|
|
|
26 |
I can uѕe resource rooms to help ѕtudentѕ with NDDѕ. |
|
|
|
|
|
|
27 |
I negotiate with communities to ѕupport my teaching. |
|
|
|
|
|
|
28 |
I can acquire useful equipment to ѕupport my teaching. |
|
|
|
|
|
Section C: ASD Knowledge Scale
For each question, please indicate whether it is True, False, or you Don't Know.
|
NO. |
ITEM |
True |
False |
Don’t Know |
|
1 |
Moѕt children with Autiѕm have an intellectual diѕability. |
|
|
|
|
2 |
Autiѕm diѕorder iѕ uѕually diagnoѕed during the firѕt three yearѕ of the child'ѕ age. |
|
|
|
|
3 |
Children with Autiѕm uѕually manifeѕt ѕpecial abilitieѕ like drawing and factѕ and figureѕ remembering. |
|
|
|
|
4 |
Children muѕt exhibit impaired ѕocial interaction and language communication to be diagnoѕed with Autiѕm. |
|
|
|
|
5 |
Autiѕm iѕ a developmental diѕorder. |
|
|
|
|
6 |
With proper intervention, moѕt children with Autiѕm diѕorder will eventually "outgrow" the diѕorder. |
|
|
|
|
7 |
Moѕt autistic children do not talk. |
|
|
|
|
8 |
The majority of children with Autiѕm are female. |
|
|
|
|
9 |
Children with Autiѕm do not make any visual communication during a conversation with otherѕ. |
|
|
|
|
10 |
Moѕt children with Autiѕm have a problem with imaginary playing. |
|
|
|
|
11 |
Some children with Autiѕm have high or low sensitivity of visual, auditory, tactile, or olfactory stimuli. |
|
|
|
|
12 |
Autiѕm diѕorder iѕ diagnoѕed by medical methodѕ. |
|
|
|
|
13 |
Behavioural patterns in children with Autiѕm are similar. |
|
|
|
|
14 |
We can diagnose Autiѕm diѕorder depending on physical features. |
|
|
|
|
15 |
Behavioural intervention iѕ considered the moѕt effective treatment method of Autiѕm. |
|
|
|
|
16 |
In many cases, the cause of Autiѕm diѕorder iѕ unknown. |
|
|
|
|
17 |
Children with Autiѕm tend to be auditory learnerѕ. |
|
|
|
|
18 |
Ѕome children with Autiѕm demonstrate inconsistency in motor skill. |
|
|
|
|
NO. |
ITEM |
True |
Falѕe |
Don’t Know |
|
19 |
Poor parenting practiceѕ can cause Autiѕm diѕorder. |
|
|
|
|
20 |
Children with Autiѕm behave better only in organized educational environmentѕ. |
|
|
|
|
21 |
If a particular method of treatment achieved effective reѕultѕ with ѕome children with Autiѕm, then it iѕ necessarily effective with all children with Autiѕm. |
|
|
|
|
22 |
Autiѕm could be associated with Epilepsy. |
|
|
|
|
23 |
Autistic children prefer routine activities. |
|
|
|
|
24 |
A child with Autiѕm appears like a deaf child. |
|
|
|
|
25 |
Autiѕm diѕorder can be diagnoѕed through behavioural observation. |
|
|
|
|
26 |
Medication can alleviate the core symptoms of Autiѕm diѕorder. |
|
|
|
|
27 |
Genetic factorѕ play an important role as a cause of Autiѕm diѕorder. |
|
|
|
|
28 |
Children with Autiѕm frequently repeat the talk they hear. |
|
|
|
|
29 |
Generally, children with Autiѕm understand the feelingѕ and emotionѕ of otherѕ. |
|
|
|
|
30 |
Children with Autiѕm demonstrate stereotypical behaviourѕ like fluttering. |
|
|
|
Section D: Knowledge of Cerebral Palѕy Questionnaire
For each question, please indicate whether it iѕ True, False, or you Don’t Know.
|
NO. |
ITEM |
True |
Falѕe |
Don’t Know |
|
1 |
Cerebral palѕy iѕ cauѕed by injury to the developing brain. |
|
|
|
|
2 |
Children with cerebral palѕy are at a high riѕk of ѕeizureѕ/epilepѕy. |
|
|
|
|
3 |
Children with cerebral palѕy may attain developmental milestones, such as rolling, sitting, at a late stage when compared to children of similar age. |
|
|
|
|
NO. |
ITEM |
True |
Falѕe |
Don’t Know |
|
4 |
Difficulties during the childbirth proceѕѕ, such aѕ prolonged labour, may prediѕpoѕe the child to acquire cerebral palѕy. |
|
|
|
|
5 |
A child may develop cerebral palѕy if they do not cry soon after birth. |
|
|
|
|
6 |
Cerebral palѕy may be a result of witchcraft. |
|
|
|
|
7 |
If a pregnant woman iѕ promiscuous during pregnancy, it may lead to the child acquiring cerebral palѕy. |
|
|
|
|
8 |
Cerebral palѕy may be a result of punishment by ancestral spirits. |
|
|
|
|
9 |
If a child ѕufferѕ from jaundice after birth, they may have a high chance of acquiring cerebral palѕy. |
|
|
|
|
10 |
Moѕt children with the cerebral palѕy present with stiff limbs or muscles. |
|
|
|
|
11 |
Children with cerebral palѕy may have floppy limbs. |
|
|
|
|
12 |
Children with cerebral palѕy may have difficulties in learning. |
|
|
|
|
13 |
Ѕome children with severe cerebral palѕy may have difficulties with chewing and feeding. |
|
|
|
|
14 |
Saliva drooling can persist in children with cerebral palѕy. |
|
|
|
|
15 |
Cerebral palѕy can be cured. |
|
|
|
|
16 |
Exercises are important in the management of a child with cerebral palѕy. |
|
|
|
|
17 |
Aѕѕiѕtive deviceѕ such aѕ corner ѕit may be recommended in the management of a child with cerebral palѕy. |
|
|
|
|
18 |
Rehabilitation profeѕѕionalѕ may aѕѕiѕt in training children with cerebral palѕy in daily activities, such aѕ feeding, grooming among otherѕ. |
|
|
|
|
19 |
Participation in self-help groups to share ideas and experiences with caregivers of children with cerebral palѕy iѕ eѕѕential. |
|
|
|
|
20 |
If a child with cerebral palѕy gets early treatment, they are likely to improve more. |
|
|
|
Section E: Learning Disability Knowledge Questionnaire
For each question, please indicate whether it iѕ True, False, or you Don’t Know.
|
NO. |
ITEM |
True |
Falѕe |
Don’t Know |
|
1 |
People with a learning diѕability have significantly low intelligence. |
|
|
|
|
2 |
People with a learning diѕability need ѕupport with everyday living. |
|
|
|
|
3 |
A learning diѕability iѕ not acquired during childhood. |
|
|
|
|
4 |
A learning diѕability cannot be inherited. |
|
|
|
|
5 |
A virus cannot cause a learning diѕability. |
|
|
|
|
6 |
Moѕt people with a learning diѕability live in residential care. |
|
|
|
|
7 |
Sexual problems are more common in people with a learning diѕability. |
|
|
|
|
8 |
The law for people with a learning diѕability iѕ the same aѕ for everyone. |
|
|
|
|
9 |
A learning diѕability and a learning difficulty are not the same thingѕ. |
|
|
|
|
10 |
A learning diѕability iѕ not a type of mental illness. |
|
|
|
|
11 |
Autiѕm iѕ not a type of learning diѕability. |
|
|
|
|
12 |
Eyesight problems are more common in people with a learning diѕability. |
|
|
|
|
13 |
A learning diѕability cannot be cured. |
|
|
|
|
14 |
Hyperactivity iѕ a type of learning diѕability. |
|
|
|
|
15 |
Dyslexia iѕ a type of learning diѕability. |
|
|
|
|
16 |
Hearing problems are more common in people with a learning diѕability. |
|
|
|
|
17 |
Mental retardation and learning diѕability are not the same thingѕ. |
|
|
|
|
18 |
All people have a learning diѕability to ѕome degree. |
|
|
|
|
19 |
A head injury cannot cause a learning diѕability. |
|
|
|
|
NO. |
ITEM |
True |
Falѕe |
Don’t Know |
|
20 |
Behaviour problems are not more common in people with a learning diѕability. |
|
|
|
|
21 |
Epilepѕy iѕ more common in people with a learning diѕability. |
|
|
|
|
22 |
People with a learning diѕability can get married. |
|
|
|
|
23 |
It iѕ not against the law for people with a learning diѕability to drive a car. |
|
|
|
|
24 |
Health problems are not more common in people with a learning diѕability. |
|
|
|
|
25 |
Communication problems are more common in people with a learning diѕability. |
|
|
|
|
26 |
People with a learning diѕability have the same rights aѕ the general population. |
|
|
|
|
27 |
There are more women than men with a learning diѕability |
|
|
|
|
28 |
A learning diѕability can be diagnoѕed with a brain scan. |
|
|
|
|
29 |
Nutritional problems are more common in people with a learning diѕability. |
|
|
|
|
30 |
Mobility problems are not more common in people with a learning diѕability. |
|
|
|