Disability Orientation and Regulatory Focus in the Assistive Technology Context: A Study of Deaf and Hard-of-Hearing Consumers
Dr. Michael Janger
Gallaudet University
AbstractWith people with disabilities (PwDs) representing 15% of the United States population, the PwD market demonstrates significant potential as a lucrative target market for businesses. Yet, empirical data is lacking on consumer behaviour among PwDs considering assistive technology products to enhance accessibility. The purpose of this study is to understand the purchase decision process through the lens of a major theory of consumer behaviour, regulatory focus. 171 deaf and hard-of-hearing individuals primarily aged 18-29 were surveyed on two empirically tested scales that measure regulatory focus and disability orientation. This survey included the viewing of a fictional advertisement about an assistive technology product. The findings supported the evidence of a relationship between disability orientation and regulatory focus. A sense of exclusion, social model acceptance, and disability pride were statistically significant predictors of either or both regulatory focus orientations with regard to assistive technology products. Also, whether the subject did/did not have a second disability was partly determinative of prevention focus. Segmentation by disability identity and regulatory focus is suggested. The findings are an important contribution to the established literature on regulatory focus, and fill a major empirical gap in marketing literature for the PwD market. The limitations to this study include the continuing theoretical evolution of disability orientation, and the limitation of the sample to a single disability type (deafness) within a single age group. Similar studies on other disability types could better establish the findings of this study.
The author would like to thank Dr. Caroline Cuny, Associate Professor of Marketing at Grenoble Ecole de Management, for her constructive criticism and guidance in the writing of this article.
Keywords: Regulatory focus, disability orientation, consumer behaviour, assistive technology, deafness, people with disabilities
Introduction
The decision-making process among consumers who evaluate, buy, and use products and services is a foundation of consumer psychology, in particular consumer behaviour. Data collected at different stages of this process inform marketers on consumer research, strategy, and product design. Theories advanced by consumer behaviour scholars such as Higgins (e.g., Higgins et al., 2001) and Aaker (e.g., Aaker & Lee, 2001) have guided the evolution and application of consumer behaviour theory in many markets across gender, ethnicity, age, religion, and other demographic types. However, there has been comparatively little scholarly analysis of consumer behaviour among people with disabilities, or PwDs, especially with regard to assistive technology products. While PwDs have benefited significantly from greater availability of assistive technology products over the last several decades, there remains a persistent sentiment among PwDs that more needs to be done to improve the quality and functionality of these products. If this is in part due to a lack of understanding of consumer behaviour patterns among PwDs who evaluate and purchase assistive technology products, then modeling this behaviour would be very invaluable for businesses and other organizations that engage with PwDs, by enabling them to improve the design, marketing, and sale of assistive technology products to PwDs, and -- importantly for PwDs themselves -- developing better assistive technology products. To address this issue, I introduce a study that assesses consumer behaviour among PwDs who evaluate assistive technology products addressing their specific disability. This study is based on prior studies that model this approach among other market segments, but never done for the PwD market segment.
As a market that represents nearly 1 of every 5 people around the world, the PwD market is one of the largest demographic segments by most measures (Brault, 2012). From a marketing and business perspective, there is sparse academic literature on the PwD market, compared to smaller but better-researched marketing segments such as the Black American segment (14% of Americans) or the Asian-American segment (6% of Americans) (Hoeffel, Rastogi, Kim, & Hasan, 2012; Rastogi, Johnson, Hoeffel, & Drewery, 2011). While much has been written about the various functional benefits of assistive technology products, little is known about the consumer psychology of PwDs as they evaluate, purchase, and use assistive technology products, and whether they are fully satisfied with these products. As noted by Rose (2017) and other historians of disability, PwDs have been marginalised by society. This marginalisation likely contributed to the undervaluation by businesses of PwDs’ economic and societal contributions as consumers, and thus a lack of understanding of PwDs’ attitudes and behaviours toward assistive technology products.
While assistive technology has delivered both expected and unexpected benefits for PwDs, there is a sense that more needs to be done to improve assistive technology products so PwDs can achieve fully equivalent functional access. Judy Heumann, a prominent disability rights activist, recounted that it has always been a challenge to find a better wheelchair that addresses certain shortcomings such as lack of wheelchair comfort, or the inconvenience of wheelchair transfer (Heumann, personal communication, January 23, 2019[1]). What are the impediments to designing, developing, and marketing “fully accessible” assistive technology? A deeper insight into business and marketing perspectives on consumer behaviour among PwDs can help shed some light on these questions from a hitherto unexplored angle.
Knowledge of PwDs’ evaluation, purchase, and usage of assistive technology products, which the present study addresses, has two immediate benefits: (1) better understanding of gaps in the specific benefits of each assistive technology product; and (2) informative and actionable information for businesses to analyse and interpret, so that they can better market to, and ultimately satisfy, the needs of PwDs. It is incumbent on disability scholars and others engaged in the PwD market to initiate efforts to address these gaps and collect and analyse data on PwD’s evaluation and utilisation of assistive technology products from the consumer behaviour perspective.
To assess the PwD’s evaluation and purchase of assistive technology products, I apply two theories in my study: regulatory focus orientation (Higgins, 1997; Higgins et al., 2001) and disability orientation (Darling, 2003, 2014). Elements of disability orientation theory are operationalised as independent variables, and the two orientations described in regulatory focus theory are the dependent variables. The model that links disability orientation and regulatory focus addresses the key question of this study: Can regulatory focus theory explain how PwDs evaluate an assistive technology product that addresses the need or want generated by the disability?
The PwDs in this study are primarily pre-lingually deaf and hard-of-hearing college students, aged 18-29. The results of the study indicate empirical evidence of a relationship between some factors of disability orientation and a PwD’s regulatory focus orientation toward an assistive technology product.
Regulatory Focus
Regulatory focus theory, first elaborated by Higgins (1997), has been frequently published and cited in academic literature, empirically proven through hundreds of studies, and often modified to be more robust in explaining the nature of the information processing of products evaluated and purchased by consumers (e.g., Aaker & Lee, 2006; Avnet & Higgins, 2006; Motyka et al., 2014). It has never been tested and modeled in the PwD market, particularly in relation to assistive technology. Any one study of regulatory focus in the PwD market will not significantly close the gap in the PwD consumer behaviour literature, but it can generate thoughtful dialogue and inquiry among disability studies scholars and spur others to study various aspects of the PwD market from the consumer behaviour perspective.
According to regulatory focus theory, a consumer focuses on either a promotion approach or a prevention approach when evaluating and purchasing a product. A consumer oriented toward a promotion focus wants something that adds value and signifies accomplishment, growth, or satisfaction, whereas a consumer oriented toward a prevention focus prioritises security and safety in his or her product evaluation and purchase decisions (Crowe & Higgins, 1997; Higgins, 1997). For example, a person decides to purchase a new car. If he/she wants more horsepower, a sporty look, and a comfortable interior in his/her new car, then he/she is promotion-focused because he/she seeks to enhance his own enjoyment by purchasing this kind of car. If he/she wants more kilometres per litre of gasoline, a more reliable engine, and a thicker body chassis in the new car, then he/she is prevention-focused because he/she seeks more security and safety by purchasing this kind of car.
A promotion orientation is based on the “fulfillment of ideals,” and success or failure is framed as a gain or non-gain, respectively. A prevention orientation is based on “oughts” or meeting obligations, and thus success or failure is framed as a non-loss or loss, respectively (Aaker & Lee, 2006; Higgins, 1997). Behaviourally, promotion-focused people experience positive feelings after success, while prevention-focused people experience “quiescence” after success. If the outcome is failure, promotion-focused people are dejected and prevention-focused people are agitated (Higgins, Shah, & Friedman, 1997).
Although the regulatory focus orientation can be chronic, people will prefer either a promotion or prevention strategy depending on the current situation. According to Crowe and Higgins (1997), the prospect of a potential loss can induce prevention-focused responses even among people with chronic promotion focus. Prospects of potential gains can induce those with chronic prevention focus to pursue a promotion strategy. Since the assistive technology industry is typically geared toward PwDs with more permanent conditions of disability, chronic regulatory focus is the more appropriate variable to evaluate for this study.
The best-known scales for measuring regulatory focus are (1) the Regulatory Focus Questionnaire (RFQ); (2) the Behavioural Inhibition/Behavioural Activation (BIS/BAS) scale; (3) the Selves questionnaire; (4) the Self-guide strength measure; and (5) the Lockwood scale. Based on Haws, Dholakia, and Bearden’s (2010) assessment of these scales, I selected the RFQ for this study for its superior predictive validity and the representativeness of either of the two types of regulatory focus orientation, despite the scale’s lack of emotional content and the past-tense orientation of its statements.
Application of Regulatory Focus to PwD Market
When applying the theory of regulatory focus to the PwD market, an insight is intuitively clear. PwDs are similar to most other consumers when it comes to basic preferences such as food, necessities, jobs, and so on. The singular difference between PwDs and people without disabilities is the desire of the former to utilise products that directly address the need or want generated by the consumer’s disability – in other words, assistive technology products. Consumers who can fully hear do not need a hearing aid, because the need to hear is satisfied. Only those who do not have full hearing may need a hearing aid. By the same logic, consumers who can fully walk do not need a wheelchair, because the need to walk is satisfied. Consumers who are paraplegic may need a wheelchair, or a product that similarly addresses their need to move on their own from point A to point B, such as a cane or walker. Thus, from the paraplegic consumer’s perspective, a wheelchair is a product that addresses the need or want generated by his or her disability.
To purchase an assistive technology product when in a promotion focus, the PwD intends to use this product as a way to enjoy and appreciate the satisfied need or want generated by the disability. If the PwD has a prevention focus when purchasing an assistive technology product, the PwD intends to use this product to minimise negative consequences arising from not filling the need or want generated by the disability itself.
However, it is not clear that regulatory focus theory alone can fully explain a PwD’s evaluation of an assistive technology product. Does a deaf person choose a hearing aid in order to enjoy the sound and enhance his/her quality of life, or to minimise the negative consequences of missing out on conversations and sounds? Or does a person with challenged walking capabilities choose one wheelchair brand over another in order to better enjoy the freedom of getting around, or to minimise the discomfort and difficulty of transferring in and out of the wheelchair?
It is difficult to answer these questions solely within the regulatory focus context, since there is sufficient anecdotal evidence that some PwDs buy an assistive technology product to appreciate a better quality of life, while others approach the same assistive technology product from the perspective that negative consequences arise from not using this product. As regulatory focus theory has been empirically proven in many different contexts, it is safe to assume that factors outside the regulatory focus framework could determine whether a PwD possesses a Promotion or Prevention orientation when evaluating or purchasing an assistive technology product. Under what conditions does a PwD pursue a Promotion focus for this product, and under what conditions does another PwD pursue a Prevention focus for this product?
Extant literature hints at some factors that might guide a PwD’s regulatory focus approach to assistive technology products that directly address his/her disability. Because their disabilities are what distinguish PwDs from the majority, non-disabled population, PwDs are sometimes viewed as not fitting into the norms and values of the majority culture. Among the reasons for the self-perception, and the perception of others, is the perceived stigma of the disability, the status of the PwD community as a minority subculture, and discrimination against members of the PwD community (e.g., Darling, 2014; Nario-Redmond, Noel, & Fern, 2013). There is empirical evidence that a person’s perception of differentness from the majority population is correlated to regulatory focus. For example, perceptions of “unfair treatment” correspond to Prevention self-regulation (Oyserman, Uskul, Yoder, Nesse, & Williams, 2007). Emotional, or affective, responses to perceived discrimination, when primed, also tended to result in Prevention self-regulation (Sassenberg & Hansen, 2007), echoing the finding that “lower-power groups” may self-regulate using a Prevention focus when communicating with “higher-power” groups (Keltner, Gruenfeld, & Anderson, 2003). Indeed, higher-power groups may pursue a Promotion focus (Sassenberg, Jonas, Shah, & Brazy, 2007).
Typology of Disability Orientation
Of the possible internal and external influences on regulatory focus orientation for any consumer, influences specific to the PwD’s decision to purchase assistive technology products are the focus of this study. While the most obvious influence is the disability itself, there are sociological and psychological influences related to the disability that also determine the PwD’s regulatory focus orientation with regard to an assistive technology product. For example, a PwD’s perception of what others in society think of his/her disability is one potential influence on his/her regulatory focus orientation.
There is little reliable empirical research in disability studies to evaluate possible influences of a PwD’s regulatory focus orientation. For example, Putnam (2005) proposed a framework for political disability identity, but did not put forth an empirical construct that would prove the efficacy of her proposed framework. Forber-Pratt, Lyew, Mueller, & Samples's (2017) review of 41 peer-review empirical studies on disability identity development found that just 22% of the studies were quantitative. This highlights the urgency of adding scientific rigour to any theorization of disability, especially in consumer psychology.
Disability orientation is one theoretical framework that is supported, to an extent, by empirical data (Darling & Heckert, 2010; Goodrich & Ramsey, 2012; Murray, 2011; Ramoso, 2017), and elements of disability orientation can be evaluated as possible predictors of regulatory focus orientation for assistive technology products. While other evolving theories at the intersection of disability and consumer psychology (Huh & Singh, 2007; Martin, Martin, Stumbo, & Morrill, 2011; Scherer, Craddock, & Mackeogh, 2011) were considered as potential independent variables in any linkage with regulatory focus theory, to date the disability orientation framework, with several published empirical studies utilising a scale developed by Darling & Heckert (2010), has potential as a valid, testable theory of disability in the consumer behaviour context.
The typology of disability orientation was developed by Darling (2003) to model how PwDs perceive their own disability, encompassing the social and medical models of disability (Oliver, 1990). Based on an earlier work by Darling (1979) on the different types of adaptations experienced by parents of children with disabilities, this framework was quantitatively tested with the Questionnaire on Disability Identity and Opportunity (QDIO) scale, with factor analysis providing initial indication that it is valid, reliable, and testable for other settings (Darling & Heckert, 2010). As a tool for empirical research in the disability market, the disability orientation framework provides an opportunity to better understand PwDs from a consumer psychology perspective, especially when evaluating and purchasing assistive technology products and services.
In Darling’s typology of disability orientation, there are two primary “orientations to disability”: the cultural majority orientation, and the minority/subcultural orientation. In the cultural majority orientation, the PwD accepts, or has access to, the norms of the non-disabled majority with respect to appearance and ability. In the minority/subcultural orientation, the PwD accepts, or has access to, the norms of the minority subculture, which is populated by PwDs and values diversity over appearance or ability. Within the two primary orientations are seven types of disability identity that reference whether the PwD has access to, or acceptance of, the values and norms of either the cultural majority or the subcultural minority. These seven types are: typicality, crusadership, affirmation, situational identification, resignation, apathy, and isolated affirmation (Darling, 2014). Descriptions of the seven types are listed in Appendix A. The first empirical testing of the disability orientation theory was administered by Darling & Heckert (2010). First, they conducted an initial qualitative study of in-depth interviews with a sample of ten individuals from small cities and rural areas to confirm the hypothesis of the existence of various orientations to disability. Upon completion of the initial qualitative study and qualitative confirmation of the hypothesis, they developed the QDIO scale to quantitatively test the hypothesis. For the QDIO, four dimensions were operationalised for measurement across 30 Likert statements, with five choices for each statement:
- Access: inclusion in, or exclusion from, society
- Identity: pride in the disability, or stigma
- Model: social model vs. medical model
- Role: level of activism in disability rights, or passivity
The QDIO was first administered to a sample of 388 PwDs across several types of disabilities. This survey produced four factors through factor analysis:
- Disability Pride (alpha = 0.78)
- Exclusion/Dissatisfaction (alpha = 0.73)
- Social Model (alpha = 0.72)
- Personal/Medical Model (alpha = 0.63)
Subsequent uses of the QDIO by other scholars generally, but not always, revealed the same factors as those by Darling & Heckert (Bogart, Lund, & Rottenstein, 2018; Goodrich & Ramsey, 2012; Murray, 2011; Ramoso, 2017). Given the limited number of use cases, lack of consistent reliability across the use cases, and mixed reproducibility of Darling & Heckert’s factors, the QDIO scale has not yet fully proven its generalisability and reliability as a scale to assess the disability orientation of PwDs. One possible explanation for the differences in the factor analyses may stem from the makeup of the type of disabilities across the samples. Different mixes of disability types may cause different factor extractions and rotations. Another explanation may be the sample sizes: the larger the sample, the less reliable the extracted factors, and less similarity with Darling & Heckert’s factors. This observation is qualified by the limited number of use cases, with only two large samples to assess. Given the status of the disability orientation framework as a still-evolving theory, the viability of this theory within the disciplines of disability studies and consumer behaviour cannot yet be ruled out. The present study brings new insights into the potential viability of this theory.
Conceptual Model and Hypothesis
The conceptual model of the relationship between disability orientation and regulatory focus in the assistive technology context is shown below as Figure 1:
Figure 1: Conceptual Model of Disability Orientation-Regulatory Focus Relationship in Assistive Technology Purchase Decision Process
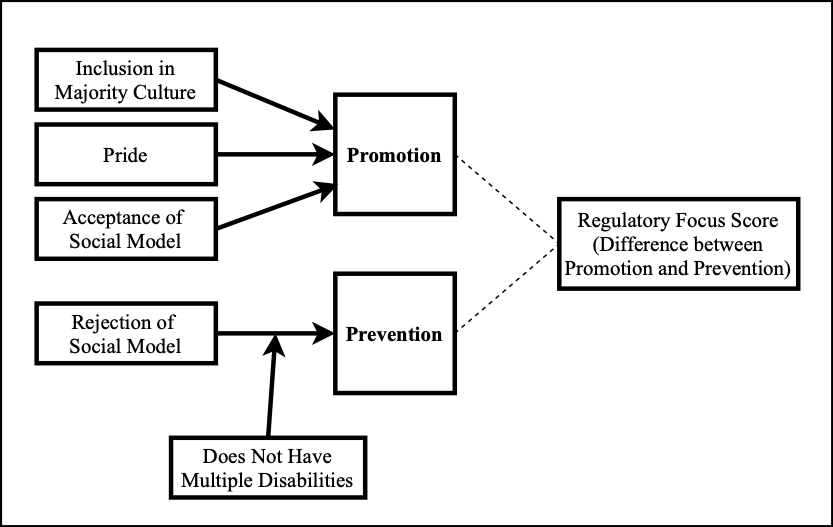
To describe the conceptual model, the independent variables that predict the Promotion dependent variable are: inclusion in majority culture; pride in the disability; and acceptance of the social model. The higher the value of any or all of these independent variables, the higher the Promotion value. The independent variable that predicts the Prevention dependent variable is the rejection of the social model, moderated by the binary value of whether the person does or does not have multiple disabilities. The higher the value of social model rejection, the higher the Prevention value. If the PwD has one type of disability, the more likely the Prevention value is higher than if the PwD has more than one type of disability.
The Promotion and Prevention dependent variables are envisioned as orthogonal (Higgins et al., 2001), so a high Promotion value does not necessarily represent a low Prevention value. However, many studies that measure regulatory focus orientation have provided a value that represents the difference between the Promotion and Prevention values, in order to measure whether a person is more Promotion-oriented and conversely less Promotion-oriented (Haws et al., 2010; Higgins et al., 2001). For that reason, RF score values are considered in our study. Yet, given the theorisation by Higgins that the two orientations are orthogonal, the validity of relying on the RF score is not definitive. Consequently, the lines between the Promotion and Prevention values and the RF score are represented in the conceptual model by dotted lines.
Based on the conceptual model, the following hypotheses are proposed:
H1: A PwD with a higher sense of inclusion in, or a lower sense of exclusion from, the majority culture, compared to other PwDs, has a stronger Promotion orientation.
H2: A PwD with a higher sense of pride in the minority subculture represented by his or her disability, compared to other PwDs, has a stronger Promotion orientation.
H3: A PwD who is more likely to accept the norms and goals of the social model, compared to other PwDs, has a stronger Promotion orientation.
H4: A PwD who is less likely to accept the norms and goals of the social model, compared to other PwDs, has a stronger Prevention orientation.
Research Design
To test the hypotheses, the QDIO and RFQ scales were merged to form the QDIO-RFQ scale. The Likert statements for both the original scales were not modified, and the sequence of the statements were kept exactly as originally written by the scales’ authors. The demographic questions in the QDIO were left unchanged, with the exception of specific questions related to the disability type being studied. In addition, a fictional advertisement for an assistive technology product directly addressing the specific type of disability was placed at the beginning of the RFQ portion of the survey.
The subjects to be surveyed for this study were next considered. One option was to survey PwDs representing different disability types. As cited earlier, prior use cases involving the QDIO surveyed multiple disability types, without providing conclusive answers due to reliability issues and inconsistency in the results of factor analysis across the cases. This is likely due to confounding factors unique to each disability type. In order to start testing the hypotheses, which assume similar consumer behaviours regardless of type of disability, the option was chosen to study one disability type: deafness. The intent was to evaluate the results and, in future studies, repeat the QDIO-RFQ for samples representing other disability types with modified demographic questions and the appropriate fictional advertisement specific to the disability type.
To effectively isolate, identify, and evaluate the independent variables from the QDIO, the QDIO portion of the survey was first administered, and the RFQ portion of the survey was administered at least a week after the completion of the QDIO portion. The week-long interval between the two survey portions was intended to eliminate potential response bias that may result from taking the RFQ too soon after the QDIO.
The Study
171 college students and recent college graduates, primarily aged 18-29 and all of whom are deaf or hard-of-hearing, participated in the study, with an incentive to complete the entire QDIO-RFQ survey for a $20 Amazon gift card. The disbursement of the gift cards was funded in part by a grant from Gallaudet University’s Office of Research Support and International Affairs. This study was approved by Gallaudet University’s Institutional Review Board (IRB).
First, the subjects were given the QDIO to complete. One week after the completion of the QDIO, they were e-mailed a link to view the fictional advertisement and then take the RFQ. The fictional advertisement showed the WakeAssure™ Vibrating Alarm Clock, by Clarity®. 154 of the 171 respondents who completed the QDIO also completed the RFQ. The entire QDIO and RFQ questionnaires, as modified for this study, are in Appendices B and C, respectively. The descriptive statistics for the study sample are in Appendix D.
Exploratory Factor Analysis of QDIO Scale
To determine whether the factors revealed by Darling and Heckert in their first use of the QDIO scale could be reproduced in this study and thus provide some validation of Darling’s disability orientation framework, an exploratory factor analysis was performed for the subjects’ responses to the 30 QDIO statements (n = 166; the remaining five subjects did not answer all 30 statements and were thus excluded from factor analysis). Since there was no information on which of the 30 QDIO items were reverse-scored by Darling and Heckert prior to their factor analysis, and no documentation of any reverse-scored items were offered in subsequent analyses of QDIO responses by other researchers, an iterative process was conducted, prior to exploratory factor analysis, to identify appropriate items in the QDIO for reverse-scoring while maintaining the reliability and consistency of the responses to the entire scale. After several cycles of this process, the appropriate items were identified for reverse-scoring, increasing the Cronbach’s alpha from 0.56 (when no items were reverse-scored) to 0.75.
An initial exploratory factor analysis was then conducted on the adjusted QDIO responses, using SPSS version 24. The Kaiser-Meyer-Olkin (KMO) value for these items was 0.677, exceeding the minimum value of 0.6 (Kaiser, 1974). Bartlett’s Test of Sphericity (Bartlett, 1954) was statistically significant at p= 0.000. Both figures indicate that the correlations among the adjusted QDIO items were suitable for factor extraction. Principal axis factoring was conducted to determine the best fit. The factoring revealed the presence of ten eigenvalues exceeding 1, cumulatively explaining 65.5% of the variance. An inspection of the scree plot, confirmed by parallel analysis, suggested a five-factor solution explaining 46.4% of the variance. Oblimin and Varimax rotations for a five-factor solution revealed similar factor structures.
Reliability tests were conducted on the five factors. The first four factors had Cronbach’s alpha coefficients of 0.753, 0.66, 0.769, and 0.637. The fifth factor, containing three items, had a Cronbach’s alpha coefficient of –0.430, indicating poor reliability. Consequently, the fifth factor was dropped, along with three other items which had factor loadings of < 0.3 and did not align to any factor. The Cronbach’s alpha coefficient for the resulting QDIO set of 24 items improved from 0.75 to 0.773, while the KMO value improved to 0.736. Running a factor analysis on the remaining 24 items resulted in the same first four factors as the five-factor solution, so a decision was made to use this four-factor solution for additional analysis.
The factors are categorised below based on assessment of the statements representing each factor, and the pattern of the responses to each of these statements:
- Factor 1: Social Model (alpha = 0.74)
- Factor 2: Exclusion/Dissatisfaction (alpha = 0.67)
- Factor 3: Pride (alpha = 0.77)
- Factor 4: Activism (alpha = 0.64)
The first 3 factors are similar, if not the same as, the factors found by Darling & Heckert in their first use of the QDIO. Table 1 below lists the results of the exploratory factor analysis of the QDIO used in our study.
Table 1: Summary of Exploratory Factor Analysis Results for QDIO Using Varimax Rotation with Kaiser Normalisation (n = 166)
| Item Code | Reversed? | QDIO Item | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
| 18 | Yes | I wish that someone would find a cure for my disability. | 0.728 | |||
| 8 | Most of my friends have disabilities. | 0.601 | ||||
| 19 | Yes | Doctors and other medical professionals know what is best for people with disabilities. | 0.562 | |||
| 21 | Yes | I try to hide my disability whenever I can. | 0.529 | |||
| 7 | Yes | I feel sorry for people with disabilities. | 0.446 | |||
| 2 | I would rather associate with disabled people than with people without disabilities. | 0.443 | ||||
| 17 | I have a lot in common with other people with disabilities. | 0.388 | 0.320 | |||
| 16 | All buildings should be accessible to people with disabilities. | 0.332 | ||||
| 13 | My disability limits my social life. | 0.624 | ||||
| 28 | I am often excluded because of my disability. | 0.545 | ||||
| 26 | People with disabilities can never fit into 'normal' society. | 0.543 | ||||
| 15 | The biggest problem faced by people with disabilities is the attitudes of other people. | 0.420 | ||||
| 14 | My disability keeps me from working. | 0.371 | ||||
| 27 | Yes | In general, I am satisfied with the quality of my life. | 0.369 | |||
| 9 | Lack of accessibility and discrimination by employers are the main reasons why disabled people are unemployed. | 0.337 | 0.354 | |||
| 6 | My disability is an important part of who I am. | 0.715 | ||||
| 3 | I am a better person because of my disability. | 0.693 | ||||
| 25 | My disability enriches my life. | 0.433 | 0.566 | |||
| 5 | I am proud of my disability. | 0.438 | 0.308 | 0.549 | ||
| 4 | Yes | If I had a choice, I would prefer not to have a disability. | 0.408 | 0.464 | ||
| 23 | I am familiar with the Disability Rights Movement and support its goals. | 0.702 | ||||
| 22 | I am familiar with the Americans with Disabilities Act (ADA) and think it is a good law.. | 0.596 | ||||
| 11 | People with disabilities need to fight for their rights more than nondisabled people do. | 0.442 | ||||
| 10 | It isn't easy for people with disabilities to be treated as 'normal.' | 0.370 | 0.385 |
Exploratory Factor Analysis of RFQ Scale
For the entire RFQ scale in the sample, the Cronbach’s alpha coefficient was 0.752. Following Higgins’ guidelines for coding each statement as either Promotion or Prevention (Higgins et al., 2001), the Cronbach’s alpha coefficients for Promotion and Prevention were 0.611 and 0.801, respectively.
Extraction of factors using principal components analysis revealed the presence of three factors with eigenvalues exceeding 1, cumulatively explaining 57.5% of the variance. Inspection of the scree plot, along with Monte Carlo PCA parallel analysis, supported a two-factor solution with a cumulative variance of 47%. The KMO value was 0.756, and Bartlett’s Test of Sphericity was statistically significant at p = 0.000. A subsequent Principal Components Analysis extraction of a fixed number of two factors, and a Varimax rotation with Kaiser normalisation, revealed the presence of the exact same items on the Prevention and Promotion factors as the items in the same factors conceptualised by Higgins et al. (2001), with the exception of Item 11, which did not align to any factor. Table 2 below lists the results of the exploratory factor analysis of the RFQ scale used in our study.
Table 2: Summary of Exploratory Factor Analysis of RFQ Using Varimax Rotation with Kaiser Normalisation (n = 154)
| Item Code | Reversed? | RFQ Item | Factor 1 | Factor 2 |
| 2 | Yes | Growing up,would you ever "crossthe line" by doing things that your parents would not tolerate? | 0.757 | |
| 4 | Yes | Did you get on your parents' nerves often when you were growing up? | 0.728 | |
| 8 | Yes | Not being careful enough has gotten me into trouble at times. | 0.688 | |
| 6 | Yes | Growing up, did you ever act in ways that your parents though were objectionable? | 0.664 | |
| 5 | How often did you obey rules and regulations that were established by your parents? | 0.444 | ||
| 3 | How often have you accomplished things that got you "psyched" to work even harder? | 0.623 | ||
| 10 | I feel like I have made progress toward being successful in my life. | 0.566 | ||
| 7 | Do you often do well at different things that you try? | 0.545 | ||
| 9 | Yes | When it comes to achieving things that are important to me, I find that I don't perform as well as I ideally would like to do. | 0.385 | |
| 1 | Yes | Compared to most people, are you typically unable to get what you want out of life? | 0.33 | 0.352 |
| 11 | Yes | I have found very few hobbies or activities in my life that capture my interest or motivate me to put effort into them. | 0.623 |
Multiple Regression of QDIO and RFQ Factors
Factor values were loaded for the four identified QDIO factors and two identified RFQ factors prior to performing multiple regression analysis.
Using Pearson product-moment correlation tests to assess relationships between the QDIO factors and the Promotion and Prevention factors prior to multiple regression, significant correlations were found for both dependent variables. The Promotion factor correlated with Exclusion & Dissatisfaction (r = 0.375, p < 0.01) and Pride (r = –0.224, p < 0.01). The Prevention factor correlated with Social Model (r = 0.241, p < 0.01) and Activism (r = 0.178, p = 0.029). Recall that for the statements in the QDIO, lower scores on the 1-to-5 Likert scale indicate agreement, and thus affinity for the QDIO factor represented by each statement. The inverse exists for the Likert-scale statements in the RFQ, with a value of 1 representing “never or seldom,” and a value of 5 representing “often.” Thus, a positive correlation between a QDIO factor and a RFQ factor indicates a higher affinity for the QDIO factor and a lower score on the RFQ factor. A negative correlation between a QDIO factor and a RFQ factor indicates a higher affinity for the QDIO factor and a higher score on the RFQ factor.
For the Exclusion & Dissatisfaction factor, a stronger sense of exclusion is correlated to a lower Promotion score, and conversely, a stronger sense of inclusion is correlated to a higher Promotion score. A stronger sense of pride in being deaf or hard-of-hearing, represented by the Pride factor, would be indicative of a higher Promotion score.
Stronger agreement with the Social Model is correlated with a lower Prevention score, while a more activist and political orientation on disability issues is also correlated with a lower Prevention score.
Because the Varimax-rotated QDIO factors are orthogonal, multicollinearity was not an issue among these factors in multiple regression.
With Promotion as the dependent variable, and the four QDIO factors as the only independent variables, the total variance explained by the Promotion regression model was 21% (F(4, 144) = 9.572, p = 0.000). Three of the four QDIO factors significantly contributed to this model: Social (beta = 0.16, p = 0.034), Exclusion & Dissatisfaction (beta = 0.371, p = 0.000), and Pride (beta = –0.222, p = 0.003). Their respective unique variances to the Promotion model were 2.5%, 13.6%, and 4.8%.
After removing two outliers which were beyond the range of normality for standardised residuals and had extreme Mahalanobis distances, the total variance explained by the Promotion model increased to 23.2% (F(4, 142) = 10.74, p = 0.000). Social (beta = 0.16, p = 0.038), Exclusion & Dissatisfaction (beta = 0.389, p = 0.000), and Pride (beta = –0.232, p = 0.002) contributed 2.4%, 15.3% and 5.3% of the unique variance in the model, respectively. Turning to the Prevention factor as the dependent variable, using the same four QDIO factors as independent variables, a Prevention regression model was developed. The total variance explained by the Prevention model with the four QDIO factors included was 11% (F(4, 144) = 4.47, p = 0.002). The QDIO factor with the only statistically significant contribution to the model was Social Model, with a unique variance of 5.7% (beta = 0.241, p = 0.003). After removing three cases with extreme Mahalanobis distances, the total variance explained by the Prevention model increased to 12.3% (F(4, 141) = 4.50, p = 0.001). The unique variance contribution of the Social Model factor increased to 7.2% (beta = 0.274, p = 0.001). The Multiple Disability Type variable significantly increased the total variance to 16.6% (F(5, 140) = 5.58, p = 0.000). The contribution of the Multiple Disability Type variable was statistically significant, with a unique variance of 4.3% (beta = –0.217, p = 0.008), indicating that those with multiple disabilities are more likely to have lower Prevention scores than those reporting one disability. The addition of this variable had little impact on the contribution of the Social Model factor, with unique variance at 5.7% and remaining statistically significant (beta = 0.247, p = 0.002).
Finally, a regression analysis of the RF score was conducted. The RF score regression model, with the four QDIO factors as the independent variables, achieved statistical significance at p = 0.045 (F(4, 144) = 2.5), with a total variance of 6.5%. Removing two cases with standardised residual scores of -3.08 and -2.85 improved the total variance to 8.5% (F(4, 142) = 3.3, p = 0.013). Adding the dichotomous Multiple Disability Type variable significantly increased the total variance explained by the regression model to 11.5%, achieving even more statistical significance at p < 0.01 (F(5, 141) = 3.67, p = 0.004).
The two independent variables which significantly contributed to the variance explained by the RF Score were Exclusion & Dissatisfaction (beta = 0.254, p = 0.002) and Multiple Disability Type (beta = 0.182, p = 0.03). Their unique variances that contributed to the model were 6.1% and 3.0%, respectively.
The result of the RF Score regression suggests that a participant who feels included in society, despite his/her deafness, would more likely have a Promotion regulatory orientation when considering whether to purchase products or services that address this disability. Similarly, a person who has other disabilities in addition to deafness would more likely have a Promotion regulatory orientation.
Canonical Correlation Analysis
To confirm the findings of the multiple regression models and provide a suggested model for segmenting the PwD market based on dimensions of disability orientation, a canonical correlation analysis was performed on the QDIO and RFQ factors, using SPSS CANCORR. Two statistically significant canonical variate pairs were revealed with respective correlations of 0.509 (s2 = 0.259, p < 0.001) and 0.229 (s2 = 0.052, p = 0.05).
Following recommended guidelines for a cutoff point of 0.55 among canonical loading values (Tabachnick & Fidell, 2013), the canonical loadings for the first pair indicate a strong relationship between the Exclusion factor and the Promotion factor, suggesting that the less excluded a PwD feels, the stronger is his/her Promotion orientation. For the second pair, the Social Model and Activism factors exhibit a significant relationship with the Prevention factor. This indicates that a PwD who is less accepting of the norms of the Social Model, and exhibits a lesser degree of activism, has a stronger Prevention orientation.
The results of the canonical correlation analysis suggest two identifiable segments of PwDs in the assistive technology market: (1) the Promotion orientation segment, represented by PwDs with a low sense of exclusion from (or high sense of inclusion in) their desired culture; and (2) the Prevention orientation segment, represented by PwDs who do not accept the social model philosophy and are not highly active in disability rights. This segmentation is mostly confirmed by the results of the multiple regression, which are similar to the results of the canonical correlation analysis except for the Activism factor, which is not a statistically significant contributor to the Prevention independent variable in the regression models.Table 3 details the results of the canonical correlation analysis.
Table 3: Canonical Correlation Analysis of the Study Sample
| Canonical Variate Pair 1 | |||
| Correlation = 0.509 | Shared Variance = 25.9% | ||
| Wilk's Lambda | Chi-Square | DF | p |
| 0.702 | 51.042 | 8 | 0.000 |
| Set 1 Canonical Loadings | Set 2 Canonical Loadings | ||
| Social Model | -0.460 | Prevention | -0.522 | Exclusion/Dissatisfaction | -0.780 | Promotion | -0.854 |
| Pride | 0.432 | ||
| Activism | -0.149 | ||
| Proportion of Variance of Set 1 Explained By Its Own Canonical Variate: 25.7% | |||
| Canonical Variate Pair 2 | |||
| Correlation = 0.229 | Shared Variance = 5.2% | ||
| Wilk's Lambda | Chi-Square | DF | p |
| 0.947 | 7.801 | 3 | 0.05 |
| Set 1 Canonical Loadings | Set 2 Canonical Loadings | ||
| Social Model | -0.610 | Prevention | -0.853 |
| Exclusion / Dissatisfaction | 0.301 | Promotion | 0.520 |
| Pride | -0.302 | ||
| Activism | -0.711 | ||
| Proportion of Variance of Set 1 Explained By Its Own Canonical Variate: 26.5% | Proportion of Variance of Set 2 Explained By Its Own Canonical Variate: 49.9% | ||
Evaluation of Hypotheses
Based on my findings, the following hypotheses are evaluated as follows:
H1: A PwD with a higher sense of inclusion in, or a lower sense of exclusion from, the majority culture, compared to other PwDs, has a stronger Promotion orientation. Exclusion is the most significant and influential predictor of the Promotion score. With statistically significant contributions of the Exclusion factor in the Promotion and RF Score regression models and the canonical correlation analysis, and the Exclusion and Inclusion factors moving in the same direction as the Promotion and Prevention orientations, respectively, Hypothesis H1 is confirmed.
H2: A PwD with a higher sense of pride in the minority subculture represented by his or her disability, compared to other PwDs, has a stronger Promotion orientation. Pride is a statistically significant predictor of the Promotion score in the Promotion regression model, with s2 = 0.053 (p < 0.01), or 22.8% of the total variance of s2 = 0.232. Although it does not predict regulatory focus orientation as well as Exclusion, it does have some influence as evidenced by its statistical significance. Since the beta of the Pride factor is negative in the Promotion regression model, it indicates that PwDs who agree with the Pride statements in the QDIO (1 = strongly agree on the 1-5 Likert scale) have a higher Promotion score.With a higher sense of Pride indicating a higher Promotion score, Hypothesis H2 is confirmed.
H3: A PwD who is more likely to accept the norms and goals of the social model, compared to other PwDs, has a stronger Promotion orientation.
H4: A PwD who is less likely to accept the norms and goals of the social model, compared to other PwDs, has a stronger Prevention orientation.
The results of the QDIO-RFQ survey provide a more complicated picture of the role of the social model in determining regulatory focus orientation. The Social Model factor is a statistically significant predictor in both the Promotion and Prevention score regression models. Yet, the Social Model betas are positive in both the Promotion and Prevention models, at 0.16 (p = 0.034) and 0.247 (p = 0.002), respectively, which would suggest that either Hypothesis H3 or Hypothesis H4 should be rejected.
In the regulatory focus literature, studies conducted to test regulatory focus theory commonly determine the regulatory focus orientation by taking the difference of the Promotion and Prevention values. The higher the value of the difference, the more likely the person is Promotion-oriented. The lower the value of the difference, the more likely the person is Prevention-oriented. The RF Score in this study is, thus, representative of the interaction of the Promotion and Prevention scores. When the RF Score is factored into the regression model, Social Model is not a significant predictor of the RF Score.
This does not rule out the utility of the Social Model as a potential predictor of regulatory focus. Since the Social Model, at this point, significantly predicts both the Promotion and Prevention scores, the size of the contribution to each score becomes more relevant. The beta for the Social Model in the Prevention model is higher than the beta for the Social Model in the Promotion model. In addition, the unique variance contributed to the Prevention model by the Social Model factor is statically significant at 5.7% (p = 0.002), while the unique variance contributed by the Social Model factor to the Promotion model is less statistically significant at 2.4% (p = 0.034) This suggests that the Social Model factor is more influential to the Prevention score than it is to the Promotion score. Since the beta of the Social Model factor in the Prevention model is positive, it indicates that the less the PwD accepts the values of the Social Model, the higher the Prevention score – or conversely, the less Promotion-oriented. Canonical correlation analysis of the entire combined sample supports this finding, with the Social Model factor having a stronger correlation with Prevention (loading = –0.61) in the second canonical variate pair than with Promotion (loading = –0.46) in the first canonical variate pair. The p-value of the canonical correlation for this second pair of variates is 0.05 for the entire combined sample, and 0.042 for the sample excluding clock owners.
While the significance of the Social Model factor as a predictor of regulatory focus is noted, it does not provide empirical evidence that the social model is a valid theory. It does, however, highlight how PwDs can accept or reject the philosophy derived from the social model. With the Social Model variable being a less statistically significant predictor of the Promotion score, and having a lower canonical loading value associated with Promotion than the loading value for Prevention, Hypothesis H3 is not confirmed.
With the Social Model being a statistically significant predictor of the Prevention score, and having a higher canonical loading value associated with Prevention than the loading value for Promotion, Hypothesis H4 is confirmed.
Theoretical and Practical Implications, and Limitations
That the disability orientation factors revealed in the current study are very similar to the factors found in Darling & Heckert’s original QDIO use case, in the context of similar supporting results from other QDIO use cases, testify to the potential viability of the disability orientation framework as a usable theory for analysis not only in consumer psychology, but also in other disciplines for which an understanding of disability self-perception is essential. Consequently, it is possible, using disability orientation theory, to model chronic regulatory focus orientation among PwDs who are evaluating and purchasing assistive technology products that address their specific disabilities. Multiple regression and canonical correlation analysis indicate that a sense of inclusion in majority culture, a sense of pride in the disability, and affinity for the norms of the social model are statistically significant predictors of regulatory focus orientation, at least for the deaf and hard-of-hearing market. An unexpected result from this study indicated that if deaf person has another disability, he/she is much less likely to be Prevention-oriented – a finding that calls for further study of people with multiple disabilities.
The results from canonical correlation analysis, supported by the multiple regression analyses, suggest the following regulatory focus profiles among PwDs in the context of the evaluation and purchase decision process for an assistive technology product:
- Promotion-Oriented PwD: Very proud of his/her disability, and does not feel a sense of exclusion from the majority culture. Assistive technology products, to this PwD, can deliver positive outcomes of excitement or enjoyment if the product does fill the disability-generated need or want. In the disability orientation typology, this suggests one of two types of disability identity: Affirmative Activism or Situational Identification (Darling, 2014).
- Prevention-Oriented PwD: Does not accept the norms and values of the social model of disability, and feels that he/she can overcome his/her disability by investing in assistive technology products that mitigate or eliminate the disability. Not being able to overcome this disability even with use of assistive technology can likely induce feelings of agitation. Consequently, the types of disability identity which would be most descriptive of prevention-oriented PwDs are Typicality, Personal Activism, or Resignation (Darling, 2014).
Up to this point, the unique attributes and characteristics of deafness have not been discussed, as they relate to the current QDIO-RFQ study on the relationship between disability orientation and regulatory focus. In a sense, this approach respects the cross-disability nature of Darling’s theory of disability orientation. Additionally, analysis of the data from the QDIO-RFQ indicate there was no relationship between the level of deafness, disability orientation, and regulatory focus. For that reason, the level of deafness as measured in decibels is not discussed in the findings on disability orientation and regulatory focus. The only identifiable contribution of deafness to the results of the QDIO-RFQ survey is its presence in the Multiple Disability Type variable, where deafness is operationalised in binary terms, with one value representing deafness as the single disability type, and the other value representing deafness as one of multiple disability types that the PwD has.
Without prior QDIO data grouped demographically by disability type, there are no prior points of comparison from where conclusions can be made about disability orientation or regulatory focus characteristics unique to deafness. If single-type studies are conducted for other disability types using the QDIO-RFQ, differences between these types and the deafness disability type could be identified and classified as characteristics or attributes unique to that type. In addition, prior studies that utilised the QDIO, particularly those by Darling & Heckert (2010) and Murray (2011) where the samples were large (n > 300) and encompassed several disability types, should be re-analysed, especially with exploratory factor analyses specific to each disability type. If differences are found in the exploratory factor analyses by disability type, they could potentially contribute to a more refined and robust version of the theory of disability orientation, and a more precise relationship between disability orientation and regulatory focus. They would also add to the academic literature specific to each disability type, such as deafness, mobility impairments, autism, blindness, and so on.
That several predictors of regulatory focus orientation toward assistive technology products could be modeled is an illustration of the role of advertising in influencing a PwD’s evaluation and purchase decision for these products. While the fictional advertisement in the QDIO-RFQ survey deliberately avoided explicit gain-framing or loss-framing in order to incorporate both regulatory focus orientations (Lee & Aaker, 2004), knowledge of the regulatory focus orientations of the target PwD market for the assistive technology product in question will be very helpful in developing more effective promotional strategies to appeal to the PwD consumer. If, for a certain assistive technology product, the targeted PwD market is primarily prevention-focused (assuming priming of chronic regulatory focus orientation for this specific product), then the promotional strategy should frame the product in the context of the dangers of potential loss as a consequence of not using the product. A promotion-focused PwD market would respond better to a promotional strategy that is gain-framed.
Whether the promotional strategy or advertisement should be gain-framed or loss-framed to appeal to the appropriate regulatory focus, it is also essential to get a sense of the PwD’s attitude (i.e. level of pride) toward their disability, his/her affinity for the social model, and whether the PwD has or does not have access to the majority culture.
While the results of the study show promise for an empirically rigourous theory of disability identity linked with consumer behaviour, there are limitations to this study. The study sample is limited to a single age group of 18-29 year olds, and to a single disability type. While broadening the age range and including other types of disabilities would have better established the validity of any predictors of regulatory focus, the risk of unique confounding factors from other age ranges and disability types make it necessary to utilise a purer sample in order to better isolate predictive factors. The results of this study can, however, be used as a baseline or a comparison point for future studies of other age ranges and/or disability types.
The risk of using a purer sample is that, in the case of deafness, there is likely to be as-yet-unidentified factors unique to deafness that may confound the results. In particular, many deaf people do not consider themselves “disabled,” and there are various references in U.S. government literature and occasional public service announcements that utilise the term “deaf or disabled.” Darling’s theory attempts to counteract this issue, by including typologies of disability that identify those who do not accept their disability, in addition to those that accept their disability (Darling, 2014).
A potential issue in interpreting the data within the conceptual model described in this study is the theoretical underpinning of the social model dimension in Darling’s typology of disability orientation. In the disability studies field, some scholars have questioned the validity of the social model of disability, or suggested revisions to the model to incorporate elements from other proposed models of disability such as the cultural model and the identity model (for a review of the models: Retief & Letšosa, 2018; for other critiques: Gabel & Peters, 2004; Shakespeare, 2006; Shildrick, 2012; Williams & Mavin, 2012). Continued theorisations of the social model in disability studies can potentially invalidate parts of the original QDIO scale used in the study. This would suggest revising the QDIO to incorporate other models of disability. This study does not measure if a PwD prefers or does not prefer the assistive technology product under consideration. It only measures the PwD’s evaluation of the product. For this reason, PwDs who reject the use of assistive technology that is used on the body, rather than provided by society, are evaluated just as equally as those who accept this type of assistive technology. It is essential to clarify that regulatory focus orientation is separate and distinct from the attitudes of PwDs toward assistive technology itself. Wang and Lee (2006), in their study on regulatory focus in preference construction, found that if a person is uninvolved in evaluating an assistive technology product for any reason, then heuristic processing takes over which influences the regulatory focus of the person. In the PwD’s case, this non-involvement can be caused by the PwD’s opinion that the focus of assistive technology should be on society and not on the individual’s body. It would be a helpful line of inquiry for further research to determine if rejecting an assistive technology product through the lens of the social model, or other models of disability, can illustrate the type of regulatory focus orientation used.
In sum, a conceptual framework that combines disability identity with regulatory focus has significant benefit for marketing strategy among businesses who plan to target PwDs with assistive technology products. A key element of this strategy is ensuring that the want and need generated by the disability is met by the assistive technology product. This requires businesses to achieve a better understanding of how PwDs decide whether or not to purchase the assistive technology product in question. When incorporating input from PwDs during the design and development of assistive technology products, it is important to go beyond seeking feedback on their use of the product toward feedback on their motivations and expectations for this product, and whether the product is viewed as providing a positive experience, or helping customers avoid potential negative experiences. This can translate to a more profitable bottom line for the business through appropriate product design and developing and executing efficient promotional strategies to connect better with the targeted PwD market. The ultimate beneficiaries are the PwDs themselves.
Suggestions for Future Research
The disability orientation framework is one of the few business-related theories in disability studies for which empirical work has been performed, and which can be applied to the study of business phenomena within the PwD market. Consequently, disability orientation, as a theory, can provide opportunities for segmenting the disability market by utilising the two primary orientations and seven types of disability identity in the framework. Applications beyond consumer behaviour theory potentially exist for this framework. Any future empirical research could result in confirmation or revision of the disability orientation framework to better describe the disability market.
Given the rich literature on regulatory focus theory, if a proven link is found between specific types of disability orientations and specific regulatory focus orientations, segmenting the PwD market by disability orientation and regulatory focus could yield a wealth of information on PwDs’ possible preferences for certain assistive technology products based on regulatory focus theory. This would enable researchers to better understand PwDs’ purchase motivations within, for example, the scarcity effect framework (Ku, Kuo, & Kuo, 2012) and/or the pursuit or lack thereof of health goals (Bui & Krishen, 2015), both of which have been analysed in the context of regulatory focus theory.
Ultimately, a better – if not yet perfect – understanding of the disability market among marketers and managers could lead to better-designed assistive technology products for PwDs, increasing the choices available to PwDs regarding products that address their disability. This, however, assumes there is data that PwDs are less than satisfied with the current products available to them that address their disability, which suggests a new avenue of research revolving around PwDs’ perceptions, as consumers, of products and services. One particularly interesting line of research could evaluate coping strategies of PwDs for assistive technology products that are not specifically designed for them, or do not completely satisfy their disability-generated need or want. How do PwDs react in this situation? Are they creative or inventive in adapting to these products, or do they avoid these products? Research on PwDs’ travel experiences provide some insight into PwDs’ possible coping strategies with assistive technology products (Ee Kim & Lehto, 2012; Kaufman-Scarborough, 2001; Poria, Reichel, & Brandt, 2011), and can be used as reference points for further research on evaluation, purchase, and usage of other products by PwDs beyond the travel industry.
Another line of research which would be particularly helpful to understanding the roles of PwDs as consumers would be a historical study of PwDs’ economic contributions to commerce and society, and how commerce has viewed PwDs through history, along the lines of writings by Rose (2017) and other disability historians. In critical disability studies, there is a strand of inquiry that explores the impact of the rise of capitalism in the 19th and 20th centuries on the quality of life of PwDs (e.g. Oliver, 1999; Russell & Malhotra, 2002). The general argument is that the rise of capitalism has worsened the quality of living among PwDs. Given the lack of empirical studies of business and consumer phenomena in the PwD market, my study may be interpreted in the context of this strand of inquiry. However, as my article focuses on a business phenomenon — more specifically, how PwDs respond to the presence of a certain assistive technology product — it does not directly touch on the sociological and economic causes of the current quality of life of PwDs in various countries including the United States. As a consequence, marginalisation of PwDs is not discussed in this article, but it is instructive to note that PwDs are indeed marginalised in the business context, not only through employment, but also in their value to marketers, market researchers, and business academics. This topic would be worthy of further study.
Conclusion
The existence of a significant and quantifiable relationship between disability orientation and regulatory focus is an important, much-needed addition to the small but promising body of empirical research on the disability orientation framework and its instrument of measurement, the QDIO. While it is not surprising that regulatory focus orientation is proven to work as a viable theory in the previously untested market of PwDs, disability orientation helped play a predictive role that explains approximately 25% of a PwD’s regulatory focus orientation toward assistive technology products, based on the results of multiple regression. Affirmative activism and situational identification are most likely associated with a Promotion orientation. Three other identity types in the disability orientation framework -- typicality, personal activism, and resignation -- are most likely associated with a Prevention orientation. The Promotion orientation segment represents PwDs who do not feel a sense of exclusion from the majority culture, and feel a stronger sense of pride in his or her disability. The Prevention orientation segment represents PwDs who reject the values of the social model and – if I accept the results of the canonical correlation analyses – are not actively involved in advocating for disability rights.
The results of the QDIO-RFQ study provide important lessons for marketers, designers, and executives, especially in businesses with little experience marketing and selling to PwDs. These businesses tend to be mainstream businesses, with its products tailored toward the non-disabled population, but which find unexpected and consistent use among PwDs. If the PwD market is sizable and significant enough to be considered a new and potentially profitable market for a business to consider entering, the findings of this study may give marketers some insights into how to sell and promote their product to this target market.
Better-directed marketing and sales efforts to the PwD market, based on a deeper and richer understanding of the interaction between disability orientation and regulatory focus, can provide businesses with a fuller, more substantive picture of the targeted PwD segment. This can potentially lead to better and more improved product designs that not only benefit the same PwD segment, but also consumers in other markets where the product is also used. This is a win-win situation: the business realises added profit to the bottom line from the PwD market and a bigger overall market through effective design and promotional strategies, and the PwD has a product that more readily satisfies the want and need generated by his/her disability and delivers a greater sense of success via positive outcome (promotion) or a more concrete sense of quiet acceptance via more successful avoidance of a negative outcome (prevention).
References
- Aaker, J. L., & Lee, A. Y. (2001). “I” Seek Pleasures and “We” Avoid Pains: The Role of Self‐Regulatory Goals in Information Processing and Persuasion. Journal of Consumer Research, 28(1), 33–49.
- Aaker, J. L., & Lee, A. Y. (2006). Understanding Regulatory Fit. Journal of Marketing Research, 43(1), 15–19.
- Avnet, T., & Higgins, E. T. (2006). How Regulatory Fit Affects Value in Consumer Choices and Opinions. Journal of Marketing Research, 43(1), 1–10.
- Bartlett, M. S. (1954). A Note on the Multiplying Factors for Various χ2 Approximations. Journal of the Royal Statistical Society. Series B (Methodological), 16(2), 296–298.
- Bogart, K. R., Lund, E. M., & Rottenstein, A. (2018). Disability Pride Protects Self-Esteem Through the Rejection-Identification Model. Rehabilitation Psychology, 63(1), 155–159.
- Brault, M. W. (2012). Americans with disabilities: 2010. Washington, D.C.: US Department of Commerce, Economics and Statistics Administration, US Census Bureau.
- Bui, M., & Krishen, A. S. (2015). So Close Yet So Far Away: The Moderating Effect of Regulatory Focus Orientation on Health Behavioral Intentions. Psychology & Marketing, 32(5), 522–531.
- Crowe, E., & Higgins, E. T. (1997). Regulatory Focus and Strategic Inclinations: Promotion and Prevention in Decision-Making. Organizational Behavior and Human Decision Processes, 69(2), 117–132.
- Darling, R. B. (1979). Families against society: A study of reactions to children with birth defects.
- Darling, R. B. (2003). Toward a Model of Changing Disability Identities: a proposed typology and research agenda. Disability & Society, 18(7), 881–895.
- Darling, R. B. (2014). Disability and identity: Negotiating self in a changing society. Lynne Rienner Publishers.
- Darling, R. B., & Heckert, D. A. (2010). Activism, Models, Identities, and Opportunities: A Preliminary Test of a Typology of Disability Orientations. Research in Social Science and Disability, 5, 203–229.
- Ee Kim, S., & Lehto, X. Y. (2012). The voice of tourists with mobility disabilities: insights from online customer complaint websites. International Journal of Contemporary Hospitality Management, 24(3), 451–476.
- Forber-Pratt, A. J., Lyew, D. A., Mueller, C., & Samples, L. B. (2017). Disability Identity Development: A Systematic Review of the Literature. Rehabilitation Psychology, 62(2), 198–207.
- Gabel, S., & Peters, S. (2004). Presage of a paradigm shift? Beyond the social model of disability toward resistance theories of disability. Disability & Society, 19(6), 585–600.
- Goodrich, K., & Ramsey, R. (2012). Are consumers with disabilities receiving the services they need? Journal of Retailing and Consumer Services, 19(1), 88–97.
- Haws, K. L., Dholakia, U. M., & Bearden, W. O. (2010). An Assessment of Chronic Regulatory Focus Measures. Journal of Marketing Research, 47(5), 967–982.
- Higgins, E. T. (1997). Beyond Pleasure and Pain. American Psychologist, 52(12), 1280–1300.
- Higgins, E. T., Friedman, R. S., Harlow, R. E., Idson, L. C., Ayduk, O. N., & Taylor, A. (2001). Achievement orientations from subjective histories of success: promotion pride versus prevention pride. European Journal of Social Psychology, 31(1), 3–23.
- Higgins, E. T., Shah, J. Y., & Friedman, R. S. (1997). Emotional Responses to Goal Attainment : Strength of Regulatory Focus as Moderator. Journal of Personality and Social Psychology, 72(3), 515–525.
- Hoeffel, E. M., Rastogi, S., Kim, M. O., & Hasan, S. (2012). The Asian population: 2010. Washington, D.C.: US Department of Commerce, Economics and Statistics Administration, US Census Bureau.
- Huh, C., & Singh, A. J. (2007). Families Travelling with a Disabled Member: Analysing the Potential of an Emerging Niche Market Segment. Tourism and Hospitality Research, 7(3–4), 212–229.
- Kaiser, H. F. (1974). An Index of Factorial Simplicity. Psychometrika, 39(1), 31–36.
- Kaufman-Scarborough, C. (2001). Sharing the Experience of Mobility-Disabled Consumers: Building Understanding Through the Use of Ethnographic Research Methods. Journal of Contemporary Ethnography, 30(4), 430–464.
- Keltner, D., Gruenfeld, D. H., & Anderson, C. (2003). Power, Approach, and Inhibition. Psychological Review, 110(2), 265–284.
- Ku, H.-H., Kuo, C.-C., & Kuo, T.-W. (2012). The Effect of Scarcity on the Purchase Intentions of Prevention and Promotion Motivated Consumers. Psychology & Marketing, 29(8), 541–548.
- Lee, A. Y., & Aaker, J. L. (2004). Bringing the Frame Into Focus: The Influence of Regulatory Fit on Processing Fluency and Persuasion. Journal of Personality and Social Psychology, 86(2), 205–218.
- Martin, J. K., Martin, L. G., Stumbo, N. J., & Morrill, J. H. (2011). The impact of consumer involvement on satisfaction with and use of assistive technology. Disability and Rehabilitation: Assistive Technology, 6(3), 225–242.
- Motyka, S., Grewal, D., Puccinelli, N. M., Roggeveen, A. L., Avnet, T., Daryanto, A., … Wetzels, M. (2014). Regulatory fit: A meta-analytic synthesis. Journal of Consumer Psychology, 24(3), 394–410.
- Murray, M. (2011). The Measurement of Beliefs, Attitudes, and Roles Related to Disability in a Sample of Rehabilitation Professionals and Clients. Indiana University of Pennsylvania.
- Nario-Redmond, M. R., Noel, J. G., & Fern, E. (2013). Redefining Disability, Re-imagining the Self: Disability Identification Predicts Self-esteem and Strategic Responses to Stigma. Self and Identity, 12(5), 468–488.
- Oliver, M. (1990). The Politics of Disablement: A Sociological Approach. New York: St. Martin’s Press.
- Oliver, M. (1999). Capitalism, disability, and ideology: A materialist critique of the Normalization principle. In A Quarter-Century of Normalization and Social Role Valorization: Evolution and Impact (pp. 163–172). University of Ottawa Press.
- Oyserman, D., Uskul, A. K., Yoder, N., Nesse, R. M., & Williams, D. R. (2007). Unfair treatment and self-regulatory focus. Journal of Experimental Social Psychology, 43(3), 505–512.
- Poria, Y., Reichel, A., & Brandt, Y. (2011). Dimensions of hotel experience of people with disabilities: an exploratory study. International Journal of Contemporary Hospitality Management, 23(5), 571–591.
- Putnam, M. (2005). Conceptualizing Disability: Developing a Framework for Political Disability Identity. Journal of Disability Policy Studies, 16(3), 188–198.
- Ramoso, T. M. S. (2017). Disability Orientation? Pride and Exclusion in College Students with Disabilities. California State University, Long Beach.
- Rastogi, S., Johnson, T. D., Hoeffel, E. M., & Drewery, M. P. J. (2011). The black population: 2010. Washington, D.C.: US Department of Commerce, Economics and Statistics Administration, US Census Bureau.
- Retief, M., & Letšosa, R. (2018). Models of disability: A brief overview. HTS Teologiese Studies/Theological Studies, 74(1), 1–8.
- Rose, S. F. (2017). No Right to be Idle: The Invention of Disability, 1840s-1930s. UNC Press Books.
- Russell, M., & Malhotra, R. (2002). Capitalism and Disability. Socialist Register, 38, 211–228.
- Sassenberg, K., & Hansen, N. (2007). The impact of regulatory focus on affective responses to social discrimination. European Journal of Social Psychology, 37(3), 421–444.
- Sassenberg, K., Jonas, K. J., Shah, J. Y., & Brazy, P. C. (2007). Why Some Groups Just Feel Better: The Regulatory Fit of Group Power. Journal of Personality and Social Psychology, 92(2), 249–267.
- Scherer, M. J., Craddock, G., & Mackeogh, T. (2011). The relationship of personal factors and subjective well-being to the use of assistive technology devices. Disability and Rehabilitation, 33(10), 811–817.
- Shakespeare, T. (2006). Disability rights or wrongs. London: Routledge.
- Shildrick, M. (2012). Critical disability studies: Rethinking the conventions for a post-conventional age. In Routledge Handbook of Disability Studies (pp. 30–41).
- Tabachnick, B. G., & Fidell, L. S. (2013). Using Multivariate Statistics. Pearson.
- Wang, J., & Lee, A. Y. (2006). The Role of Regulatory Focus in Preference Construction. Journal of Marketing Research, 43(1), 28–38.
- Williams, J., & Mavin, S. (2012). Disability as Constructed Difference: A Literature Review and Research Agenda for Management and Organization Studies. International Journal of Management Reviews, 14(2), 159–179.
Appendices
Appendix A: The Seven Types of Disability OrientationAppendix B: Questionnaire on Disability Identity and Opportunity (1st Part of QDIO-RFQ)
Appendix C: Regulatory Focus Questionnaire (2nd Part of QDIO-RFQ)
Appendix D: Demographics of Participants in The Study
APPENDIX A: THE SEVEN TYPES OF DISABILITY ORIENTATION
The seven types of disability orientation are summarily described as follows (Darling, 2003, 2014):
- Typicality: Accept the norms and values of the cultural majority “with regard to appearance and/or ability” and adopt lifestyles similar to those without disabilities. This type was labeled in Darling’s earlier version of the disability orientation typology (Darling, 2003) as “normalisation.”
- Personal Activism: Accept the norms and values of the cultural majority, yet do not have access to the lifestyle associated with the majority. Usually, people with this type get involved in the minority subculture associated with the disability, as a means to achieve typicality.
- Affirmative Activism: Accept the norms and values of the minority subculture associated with their disability, but do not make concerted attempts at typicality in the cultural majority. At times, people with this type can seek access to participation in the cultural majority. They usually view their disability in positive terms, and as their primary identity.
- Situational Identification: Adopt whatever identity is appropriate at any given time, whether it is to pursue full inclusion in the majority culture and adopt its lifestyle, or at other times to interact with members of the minority subculture and reject typicality.
- Resignation: Desire typicality, but have no access to the majority culture, and do not have access to, or accept the, norms of the minority subculture.
- Apathy: Have access to either the majority culture or minority subculture, but are either unaware of or do not have the desire for acceptance to either culture.
- Isolated Affirmative Activism: No access to either the majority culture or minority subculture, but accept the norms and values of the subculture. People with this type are initially not aware of the existence of a disability subculture, but have ideas that are affirmative of this subculture. Upon awareness of the subculture’s existence, they would join it.
APPENDIX B: QUESTIONNAIRE ON DISABILITY IDENTITY AND OPPORTUNITY (1ST PART OF QDIO-RFQ)
Please read each of the following statements and click on the button that best represents your level of agreement:
| Strongly Agree | Strongly Disagree | ||||
| I don't think of myself as a disabled person. | ○ | ○ | ○ | ○ | ○ |
| I would rather associate with disabled people than with people without disabilities. | ○ | ○ | ○ | ○ | ○ |
| I am a better person because of my disability. | ○ | ○ | ○ | ○ | ○ |
| If I had a choice, I would prefer not to have a disability. | ○ | ○ | ○ | ○ | ○ |
| I am proud of my disability. | ○ | ○ | ○ | ○ | ○ |
| My disability is an important part of who I am. | ○ | ○ | ○ | ○ | ○ |
| I feel sorry for people with disabilities. | ○ | ○ | ○ | ○ | ○ |
| Most of my friends have disabilities. | ○ | ○ | ○ | ○ | ○ |
| Lack of accessibility and discrimination by employers are the main reasons why disabled people are unemployed. | ○ | ○ | ○ | ○ | ○ |
| It isn't easy for people with disabilities to be treated as "normal." | ○ | ○ | ○ | ○ | ○ |
| People with disabilities need to fight for their rights more than nondisabled people do. | ○ | ○ | ○ | ○ | ○ |
| The reason most people with disabilities are unemployed is that they are not able to do the jobs that are available. | ○ | ○ | ○ | ○ | ○ |
| My disability limits my social life. | ○ | ○ | ○ | ○ | ○ |
| My disability keeps me from working. | ○ | ○ | ○ | ○ | ○ |
| The biggest problem faced by people with disabilities is the attitudes of other people. | ○ | ○ | ○ | ○ | ○ |
| All buildings should be accessible to people with disabilities. | ○ | ○ | ○ | ○ | ○ |
| I have a lot in common with other people with disabilities. | ○ | ○ | ○ | ○ | ○ |
| I wish that someone would find a cure for my disability. | ○ | ○ | ○ | ○ | ○ |
| Doctors and other medical professionals know what is best for people with disabilities. | ○ | ○ | ○ | ○ | ○ |
| People with disabilities need to learn to adjust to living in a world in which most people are not disabled. | ○ | ○ | ○ | ○ | ○ |
| I try to hide my disability whenever I can. | ○ | ○ | ○ | ○ | ○ |
| I am familiar with the Americans with Disabilities Act (ADA) and think it is a good law. | ○ | ○ | ○ | ○ | ○ |
| I am familiar with the Disability Rights Movement and support its goals. | ○ | ○ | ○ | ○ | ○ |
| People should try to overcome their disabilities. | ○ | ○ | ○ | ○ | ○ |
| My disability enriches my life. | ○ | ○ | ○ | ○ | ○ |
| People with disabilities can never fit into "normal" society. | ○ | ○ | ○ | ○ | ○ |
| In general, I am satisfied with the quality of my life. | ○ | ○ | ○ | ○ | ○ |
| I often am excluded from activities because of my disability. | ○ | ○ | ○ | ○ | ○ |
| The people I care about always include me in activities I am able to enjoy. | ○ | ○ | ○ | ○ | ○ |
| The most important thing for people with disabilities is to learn to accept what they cannot change. | ○ | ○ | ○ | ○ | ○ |
Please answer the following questions by clicking on the description that applies to you:
What is your gender?
○ Male
○ Female
*
What is your age, in years?
___________________________
What is your marital status?
○ Never married
○ Married
○ Separated or divorced
○ Widowed
What is your employment status?
○ Work full time
○ Work part time
○ Unemployed or homemaker
○ Student
○ Retired
Where do you live?
○ Small town
○ Rural area
○ Medium-sized or small city
○ Suburb of a large or medium-sized city
○ Large city
What is the highest level of school you have completed?
○ Less than high school
○ High school
○ Some college
○ College
○ Some graduate school
○ Graduate school
Display this question:
If What is the highest level of school you completed? = Some college
Or What is the highest level of school you completed? = College
Or What is the highest level of school you completed? = Some graduate school
Or What is the highest level of school you completed? = Graduate school
What college or university did you, or do you currently, attend?
________________________________________________________________
What is the nature of your disability, handicap, or impairment? (If you have more than one, please check as many as apply.)
○ Mobility (difficulty in movement)
○ Vision
○ Hearing
○ Speech
○ Cognitive (Difficulty in thinking)
○ Cosmetic (Difference in appearance or size)
○ Other - please specify
Describe your deafness in terms of decibel (dB) loss for each of your ears. (If you do not know your specific level, please give your best estimate, or leave blank.)
| Less than 21 dB (None or Slight) | 21-45 dB (Mild) | 46-65 dB (Moderate) | 66-90 dB (Severe) | 91 dB or more (Profound) | |
| Left ear | ○ | ○ | ○ | ○ | ○ |
| Right ear | ○ | ○ | ○ | ○ | ○ |
How long have you had your disability, handicap, or impairment? (If you have more than one, please check the time that describes the condition you have had the longest.)
○ Since birth
○ Less than 5 years
○ 5-10 years
○ More than 10 years
How much assistance do you need with activities of daily living (like bathing, dressing, shopping, and cooking)?
○ I need assistance with all activities.
○ I need assistance with some activities.
○ I don't need any assistance.
About how often do you engage in social activities outside of your home, like visiting friends or eating out in restaurants?
○ More than once a week
○ Once or several times a month
○ Occasionally, less than once a month
○ Rarely or never
Have you ever participated in a demonstration, written a letter to your congressional representative, or engaged in another activity to try to increase the opportunities available to people with disabilities?
○ Yes, many times
○ Yes, a few times
○ Yes, once
○ No, never
Please check the activities in which you participate at least once a month (check all that apply):
☐ Talking on the phone with family, friends, or acquaintances
☐ Using a computer to communicate by email
☐ Using a computer to access disability-related websites on the computer
☐ Using a computer to access other websites
☐ Going to meetings or other activities sponsored by disability-related organizations
☐ Going to meetings or activities of other organizations
☐ Attending religious services
☐ Reading magazines or newsletters from disability-related organizations
Please check the category that describes your total annual household income:
○ Under $25,000
○ $25,000 - $50,000
○ $50,000 - $100,000
○ Over $100,000
Please check the category or categories that best describe your racial/ethnic background:
○ European American (white)
○ African American
○ Latino or Hispanic
○ Native American or Indian
○ Asian American
○ Other
YOU HAVE REACHED THE BOTTOM OF THE SURVEY. PLEASE REVIEW YOUR ANSWERS. WHEN YOU ARE SATISFIED WITH YOUR ANSWERS, CLICK "NEXT" TO PROCEED.
End of Block: QDIO
Start of Block: Partial Answer
IT APPEARS YOU DID NOT ANSWER ALL THE QUESTIONS IN THIS SURVEY.
DID YOU MISS A QUESTION? CLICK ON "NEXT" TO TAKE YOU BACK TO THE SURVEY. REVIEW YOUR ANSWERS AND ANSWER ANY QUESTION(S) YOU MISSED. THEN CLICK ON "NEXT" TO FINISH YOUR SURVEY AND SUBMIT YOUR ANSWERS.
DO YOU PREFER NOT TO ANSWER ONE OR MORE QUESTIONS? THAT'S OKAY. CLICK ON "NEXT" TO TAKE YOU BACK TO THE SURVEY, AND THEN CLICK ON "NEXT" TO FINISH YOUR SURVEY AND SUBMIT YOUR ANSWERS.
APPENDIX C: REGULATORY FOCUS QUESTIONNAIRE
(2ND PART OF QDIO-RFQ)
Welcome back, and thank you for taking the time to do this 2nd survey.
On the next page is an advertisement. You can view it for as long as you want (but no more than 5 minutes) before moving on to the survey. Please click on the "Next" button below to view the advertisement.
NOTE: This is not an actual advertisement. Although it is about a real product, this advertisement was designed by the researchers solely for purposes of an academic study, and this product was selected specifically to meet the study's criteria. This advertisement has not been viewed, endorsed, or approved by the manufacturer of the selected product.
When you have finished viewing the advertisement, please click the "Next" button below at any time to start the survey. (The survey will automatically start after 5 minutes, if you have not clicked "Next".)
This set of questions asks you HOW FREQUENTLY specific events actually occur or have occurred in your life. Please indicate your answer to each question by clicking on the appropriate answer.
| Never or Seldom 1 |
2 | Sometimes 3 |
4 | Very Often 5 |
|
| Compared to most people, are you typically unable to get what you want out of life? | ○ | ○ | ○ | ○ | ○ |
| Growing up, would you ever "cross the line" by doing things that your parents would not tolerate? | ○ | ○ | ○ | ○ | ○ |
| How often have you accomplished things that got you "psyched" to work even harder? | ○ | ○ | ○ | ○ | ○ |
| Did you get on your parents nerves growing up? | ○ | ○ | ○ | ○ | ○ |
| How often did you obey rules and regulations that were established by your parents? | ○ | ○ | ○ | ○ | ○ |
| Growing up, did you ever act in ways your parents found we objectionable? | ○ | ○ | ○ | ○ | ○ |
| Do you often do well at different things that you try? | ○ | ○ | ○ | ○ | ○ |
| Not being careful enough has gotten me into trouble at times. | ○ | ○ | ○ | ○ | ○ |
| When it comes to achieving things that are important to me, I find that I don't perform as well as I ideally would like to do. | ○ | ○ | ○ | ○ | ○ |
| I feel like I have made progress toward being successful in my life. | ○ | ○ | ○ | ○ | ○ |
| I have found very few hobbies or activities in my life that capture my interest or motivate me to put effort into them. | ○ | ○ | ○ | ○ | ○ |
Make sure you have answered ALL questions. You will get an error message if you click on "Next" without answering all questions.
Click on "Next" when finished.
Do you own, or have you at some point in the past owned, the exact alarm clock that was shown in the advertisement at the beginning of this survey? The advertisement is shown again below for your reference. Please answer "Yes" or "No", and then click on "Next" to finish and submit the survey.
○ Yes
○ No
APPENDIX D: DEMOGRAPHICS OF PARTICIPANTS IN THE STUDY
| Number of Participants in Sample (n = 171) | |
| Completed QDIO | 171 | Completed RFQ | 154 | Gender (n = 171) |
| Male | 66 |
| Female | 105 |
| Age, Mean (n = 171) | |
| Male | 22.6 |
| Female | 22.8 |
| All | 22.7 |
| Date of Onset of Disability (n = 171) | |
| At Birth | 133 |
| More than 10 years ago | 28 |
| Less than 10 years ago | 10 |
| Number of Disability Types (n = 171) | |
| Deafness Only | 139 |
| Deafness plus at least one other disability | 32 |
| Level of Deafness (Percentage of n = 171) | |
| Profoundly deaf | 60% |
| Less than profoundly deaf | 40% |
| Require Assistance (n = 171) | |
| No | 154 |
| Yes | 17 |
| Owns or Owned Clock in Advertisement (n = 154) | |
| No | 111 |
| Yes | 33 |
| Race (n = 170) | |
| European American (White) | 121 |
| African American | 14 |
| Latino or Hispanic | 13 |
| Asian American | 12 |